All published articles of this journal are available on ScienceDirect.

Prevalence of Patients Receiving Publicly Funded Renal Replacement Therapy in Brazil: Regional Inequities and Costs
Authors Info & Affiliations
Abstract
Introduction:
In recent years, the number of patients with end-stage renal disease has rapidly increased worldwide. In Brazil, recent surveys have undisclosed a trend towards an increase in the prevalence of this condition.
Aims and Objectives:
This study aimed at describing the prevalence of patients with end-stage renal disease (ESRD) receiving publicly funded dialysis in Brazil.
Methods asnd Materials:
Data concerning the prevalence and mortality of patients with ESRD being provided renal replacement therapy by the SUS from 2008 to 2013 were collected at the DATASUS databank (www2.datasus.gov.br), the Authorization System for High Complexity/Cost Procedures (APAC) database, the SUS Ambulatory Information System (SIA) and the Mortality Information System (SIM) database.
Results:
From 2008 to 2013 there was a 25% increase in the absolute number of hemodialysis sessions (10,022,962; 12,561,623). This resulted in an estimated overall increase of 18% in the ratio of patients on hemodialysis per million population (352 pmp; 416 pmp). There were considerable differences among Brazilian States regarding the prevalence of patients with ESRD on hemodialysis. In 2013, the prevalence ranged from 173 pmp (State of Amazonas) to 531 pmp (State of Minas Gerais). The leading Brazilian States, in absolute number of patients, were São Paulo (19,301), Minas Gerais (10,940) and Rio de Janeiro (8,510), all of them in the southeast region. In 2013, the overall mean mortality rate was 18.4%. From 2008 to 2013, the renal transplantation rate increased from 35.2 to 41.6 transplants per year per million inhabitants. In 2013, hemodialysis was the most frequent modality of therapy, corresponding to 87.1% of the cases, followed by CAPD (9.2%) and APD (3.7%).
Conclusion:
In Brazil, chronic kidney disease is steadily increasing in prevalence and rapidly becoming a major public health concern. Therefore, policies towards prevention and strategies to avoid underdiagnose and assure broad access to renal replacement therapy should be strengthened nationwide.
1. INTRODUCTION
During the past decades Brazil has undergone rapid changes in major social and economic determinants of health [1, 2]. Concurrently, Brazil has also experienced a rapid demographic transition resulting in an increase in the number of adults and elderly people [3]. This has led to a shift in the causes of morbidity and mortality in the Brazilian population from infectious diseases to chronic non-communicable diseases (CNCD) [3, 4].
In recent years, the number of patients with end-stage renal disease (ESRD) has rapidly increased worldwide resulting in a global public health problem [4-6]. In Brazil, recent surveys have undisclosed a trend toward an increase in the prevalence of this condition [7-11].
To face this challenge, the Brazilian public health system, Sistema Único de Saúde (SUS), has increased its efforts to accomplish the State duty of providing universality of coverage to all Brazilian citizens enforcing primary healthcare policies. In spite of that, Brazil still faces serious problems involving equity, quality, and efficiency of healthcare services [1, 2]. In this scenario, knowledge on the prevalence of patients on chronic dialysis treatment can be decisive in the development of more effective healthcare policies [12].
Therefore, this study aimed at describing the prevalence of patients with ESRD receiving publicly financed dialysis in Brazil from 2008 to 2013.
2. PATIENTS AND METHODS
Data concerning the prevalence and mortality of patients with ESRD being provided renal replacement therapy by the SUS from 2008 to 2013 were collected at the DATASUS databank (www2.datasus.gov.br), the Authorization System for High Complexity/Cost Procedures (APAC) database, the SUS Ambulatory Information System (SIA) and the Mortality Information System (SIM) database.
The absolute number of dialysis sessions was calculated considering the total number of reimbursement registries via APAC. The Brazilian government pays hemodialysis sessions on a fixed rate of 3 times per week with the possibility of an extra session every week under exceptional circumstances. Therefore, this study considered that on average one patient would undertake 150 hemodialysis sessions per year. Hence, we have estimated the absolute number of patients on hemodialysis by dividing the total annual number of sessions on a given location by 150.
Other variables analyzed were the region of residence in Brazil, type of renal unit (private vs. public), type of dialysis treatment (hemodialysis, peritoneal dialysis, renal transplantation) and costs. The resulting data were analyzed in September 2014.
This study produced no interventions and the privacy of the researched subjects and the confidentiality of their personal information were handled in accordance with the ethical principles of the Declaration of Helsinki.
3. RESULTS
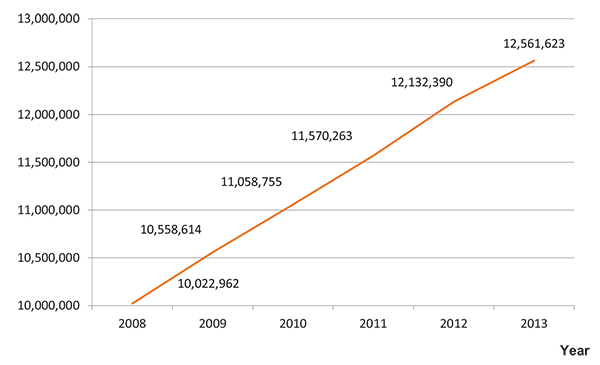
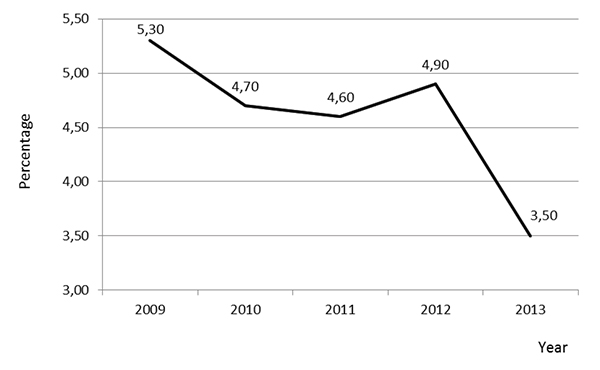
From 2008 to 2013 there was a 25% increase in the absolute number of hemodialysis sessions (10,022,962; 12,561,623; Fig. (1)). This resulted in an estimated overall increase of 18% in ratio of patients on hemodialysis per million population (352 pmp; 416 pmp; Fig. (2) and Table 1). Annually, the mean increase in the number of patients was of 4,6%, (Fig. 3).
| Federal State | Population in 2013 | Estimated Patients on Hemodialisys | Prevalence per Million Inhabitants | Mortality | Mortality Rate (%) |
|---|---|---|---|---|---|
| Acre | 776,463 | 214 | 276 | 64 | 30.0 |
| Alagoas | 3,300,938 | 1,365 | 414 | 395 | 28.9 |
| Amapa | 734,995 | 180 | 245 | 36 | 20.0 |
| Amazonas | 3,807,923 | 657 | 173 | 93 | 14.2 |
| Bahia | 15,044,127 | 5,297 | 352 | 855 | 16.1 |
| Ceara | 8,778,575 | 3,539 | 403 | 532 | 15.0 |
| Distrito federal | 2,789,761 | 1,055 | 378 | 167 | 15.8 |
| Espirito santo | 3,839,363 | 1,947 | 507 | 335 | 17.2 |
| Goias | 6,434,052 | 3,167 | 492 | 483 | 15.2 |
| Maranhao | 6,794,298 | 1,781 | 262 | 115 | 6.5 |
| Mato grosso | 3,182,114 | 1,327 | 417 | 224 | 16.9 |
| Mato grosso do sul | 2,587,267 | 1,123 | 434 | 277 | 24.7 |
| Minas gerais | 20,593,366 | 10,940 | 531 | 2,252 | 20.6 |
| Para | 7,999,730 | 1,556 | 195 | 257 | 16.5 |
| Paraiba | 3,914,418 | 1,094 | 279 | 285 | 26.1 |
| Parana | 10,997,462 | 4,128 | 375 | 825 | 20.0 |
| Pernambuco | 9,208,551 | 4,368 | 474 | 527 | 12.1 |
| Piaui | 3,184,165 | 1,463 | 459 | 212 | 14.5 |
| Rio de janeiro | 16,369,178 | 8,510 | 520 | 1,292 | 15.2 |
| Rio grande do norte | 3,373,960 | 1,504 | 446 | 301 | 20.0 |
| Rio grande do sul | 11,164,050 | 5,181 | 464 | 1,673 | 32.3 |
| Rondonia | 1,728,214 | 537 | 311 | 136 | 25.3 |
| Roraima | 488,072 | 145 | 297 | 5 | 3.4 |
| Santa catarina | 6,634,250 | 2,218 | 334 | 547 | 24.7 |
| Sao paulo | 43,663,672 | 19,301 | 442 | 3,364 | 17.4 |
| Sergipe | 2,195,662 | 681 | 310 | 99 | 14.5 |
| Tocantins | 1,478,163 | 398 | 269 | 64 | 16.1 |
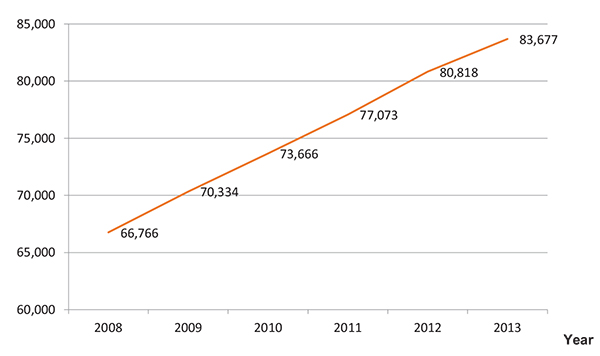
| Total | 201,062,789 | 83,677 | 416 | 15,415 | 18.4 |
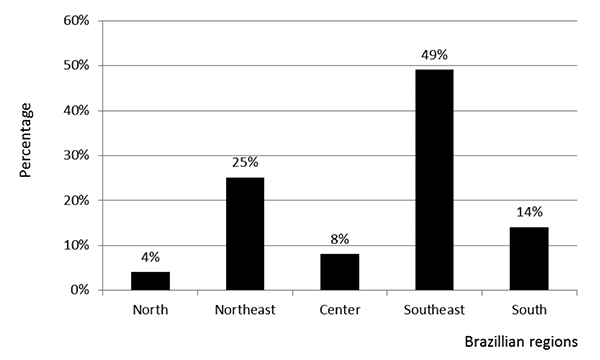
There were considerable differences among Brazilian States regarding the prevalence of patients with ESRD on hemodialysis. In 2013, the prevalence ranged from 173 pmp (State of Amazonas) to 531 pmp (State of Minas Gerais). The leading Brazilian States, in absolute number of patients, were São Paulo (19,301), Minas Gerais (10,940) and Rio de Janeiro (8,510), all of them in the southeast region, (Fig. 4).
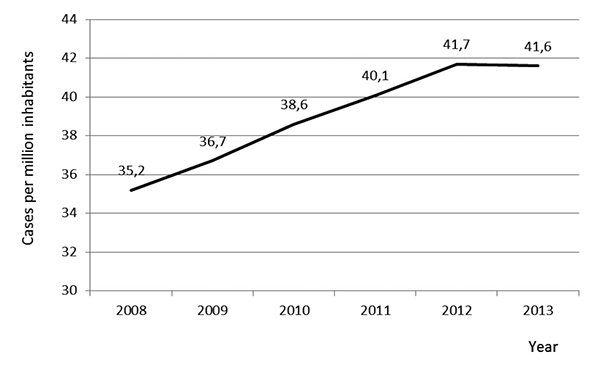
The mean annual renal transplantation rate per million inhabitants increased from 35.2 pmp in 2008 to 41.6 pmp in 2013, (Fig. 5 and Table 1). In 2013, the overall mean mortality rate was 18.4%, (Table 1). In this same year, 95% of the total expenses with publicly funded dialysis sessions were allocated to treat patients on private facilities.
In other words, only 5% of the expenses were spent on public dialysis facilities. In 2013, the estimated total expenses to cover dialysis and catheters costs approximated 500 million US dollars. Compared to 2008, this represented an increase of 67% in costs (R$1,344,793,917 to R$2,253,434,171).
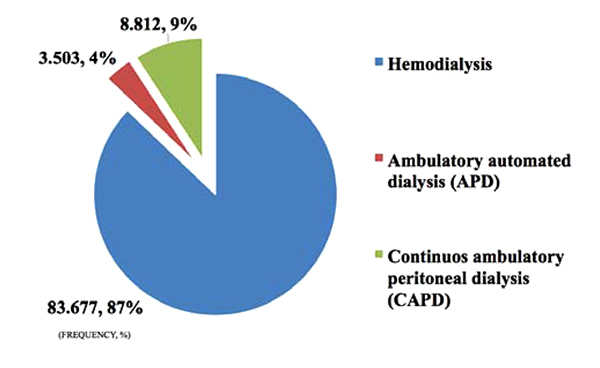
In 2013, hemodialysis was the most frequent modality of renal replacement therapy used, corresponding to 87.1% of the cases, followed by CAPD (9.2%) and APD (3.7%), (Fig. 6).
4. DISCUSSION
Currently it is believed that the underlying determinants of chronic diseases are strictly associated with the social, economic and cultural changes seen worldwide in the late decades [13]. Globalization, unrestricted urbanization, population ageing, improved access to fast food and continuous exposure to unhealthy habits are some of the factors believed to have contributed to increase the burden of chronic non-communicable diseases (CNCD) especially in low and middle-income countries like Brazil [14-17]. In spite of that, epidemiological data regarding the burden of CNCD are still scarce. In Brazil, the Brazilian Society of Nephrology [10] regularly estimates the total number of patients on dialysis based on surveys, however this country still lacks an official public registry of ESRD patients on dialysis. Therefore this study aimed at scrutinizing databanks obtained from the Brazilian Ministry of Health focusing on the prevalence and mortality of patients with ESRD on publicly funded renal replacement therapy in Brazil.
From 2008 to 2013 there was an increase in the order of 6% in number of inhabitants in Brazil (189 million to 201 million inhabitants). In this meanwhile, in contrast, it was observed a 25% increase in the absolute number of publicly funded hemodialysis sessions in Brazil. This resulted in an estimated overall increase of 18% in the ratio of patients on hemodialysis per million population in five years (352 pmp; 416 pmp). In spite of this dramatic increase, the prevalence of patients under dialysis treatment in Brazil is still far from what is seen in developed countries as the United States, where the rate of patients on hemodialysis per million population is about 1,200 [18, 19].
Considerable local differences across Brazilian States regarding the prevalence (ranging from 173 pmp to 531 pmp) and mortality (ranging from 3,4% to 32.3%) of patients with ESRD on hemodialysis was also seen. These differences suggest the existence of intrinsic regional difficulties to properly identify and treat patients with ESRD in several Brazilian regions and also raise suspicion on underdiagnose and sub notification practices. Part of these differences could also be due to economical inequities between Brazilian States once higher prevalence were specially observed in the most economic developed areas in contrast to the poorest States of Brazil.
In Brazil, only about 16% of the total dialysis sessions are provided by private funds, in spite of this, most of the current publicly funded dialysis sessions occur on private facilities (95% private versus 5% public). This suggests that the practices and results obtained in the treatment of the ESRD in Brazil, despite largely dependent on public funds, is critically influenced by the decisions and the quality of care provided by the private sector. This also helps to explain why despite the large territorial extension, peritoneal dialysis is the modality of choice for only about 13% of the Brazilian population under dialysis. Brazil has just taken its initial steps in establishing comprehensive policies encouraging peritoneal dialysis across the country. Therefore, the Brazilian current results on peritoneal dialysis are still hugely influenced by economic and historical practices rather than a structured plan of action tailored in accordance to its population needs.
CONCLUSION
Chronic kidney disease is increasing in prevalence and therefore it is rapidly becoming a major public health concern in Brazil. Policies for its prevention and treatment should be nationwide strengthened aimed at reducing regional inequities regarding the detection of ESRD and access to renal replacement modalities across different locations in Brazil.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
No Animals/Humans were used for studies that are base of this research.
CONSENT FOR PUBLICATION
Not applicable.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared None.

