All published articles of this journal are available on ScienceDirect.

Comparison of Acuseal and Standard ePTFE Vascular Grafts for Hemodialysis: A Retrospective Case Series
Abstract
Background:
Grafts, which allow early cannulation have been increasingly used to avoid starting dialysis via tunneled hemodialysis catheters. As we noted graft failures in patients with early cannulation grafts, we reviewed the outcome of these grafts and compared it to ePTFE grafts.
Materials and Methods:
We retrospectively analyzed time to first intervention, primary and secondary patency rates as well as the number of interventions needed to maintain patency in patients who received an early cannulation graft (GORE® ACUSEAL, acuseal) or an ePTFE (GORE-TEX®) vascular graft between January 2016 and November 2017 in our medical center.
Results:
12 patients who had received an acuseal vascular graft were compared with 13 patients with an ePTFE vascular graft. The mean time to first intervention was similar in both groups. On average 0.33 interventions per graft were needed per month to maintain patency in the acuseal group, and 0.08 in the ePTFE group (p = 0.02). The primary patency rate did not differ significantly between the groups. The secondary patency rate at the end of the observation period was significantly worse in the acuseal group (p = 0.02). Four acuseal grafts were lost after a mean of 202 days, whereas none of the ePTFE grafts was lost.
Conclusion:
Our data is consistent with our clinical impression of an increased number of interventions and lower longevity of the acuseal vascular graft. These data need conformation in a larger cohort.
1. INTRODUCTION
In recent decades, the dialysis population has changed considerably with a heightened prevalence of diabetes mellitus, an increasing cardiovascular risk and rising age [1]. The native fistula is the vascular access of choice for hemodialysis, but with a changing dialysis population the vascular prerequisites for the formation of native accesses are deteriorating. The usage of tunneled dialysis catheters is associated with a higher incidence of complications like infections, impaired functional status and a higher all-cause mortality [2]. Additionally, the need for dialysis is often urgent and there might not be enough time for the maturation of a native fistula. Therefore, the usage of an early cannulation graft like the acuseal vascular graft, which can be cannulated within 24 hours of implantation would be of significant clinical benefit.
The acuseal vascular graft is a tri-layer graft consisting of an abluminal expanded Polytetra-Fluoroethylene (ePTFE) layer, an elastomic layer and a luminal ePTFE layer with a CBAS® (Carmeda® BioActive Surface) Heparin surface (W. L. Gore & Associates). This construction allows for immediate cannulation and hinders cannulation bleeding. Recent reports about the use of acuseal vascular grafts have shown patency rates in the range of other vascular grafts, but to our knowledge studies comparing the acuseal vascular graft with other vascular grafts are lacking [3, 4]. Here, we report our exper-ience with acuseal vascular grafts in comparison with standard ePTFE grafts in a retrospective case series.
2. METHODS
This retrospective observational case study was carried out in our institute in patients who underwent surgical implantation of an acuseal or an ePTFE vascular graft as part of an arteriovenous fistula creation between the 1st of January 2016 and the 30th of November 2017. The decision, whether an acuseal or an ePTFE vascular graft was implanted was made by the vascular surgeon in charge. Acuseal vascular grafts were preferentially used when immediate dialysis was required. The surgical procedures were similar for the implantation of acuseal and ePTFE grafts. All patients who received an acuseal vascular graft and an equivalent number of patients with an ePTFE vascular graft were identified by a vascular surgeon using surgical protocols. Subsequently, data on patient demographics, vascular access history, number of percutaneous angioplasties and surgical interventions necessary to maintain patency of their vascular access were extracted from the electronic medical system of the hospital. 31 patients were screened for inclusion in the study. Seven patients had to be excluded, because of graft infection or because their shunt was a combination of an acuseal and an ePTFE graft. One patient consecutively and separately had an acuseal and then an ePTFE vascular graft and was included in both study groups. Therefore, in total 12 acuseal and 13 ePTFE vascular grafts were included in the study. The end of the observation period was defined as the date at which the graft was no longer in use (i.e. the date of kidney transplantation, death or graft loss) or the prespecified study end (20th of January 2018). Primary patency was defined as the intervention-free survival of the vascular graft. Secondary patency was defined as the time without graft loss including grafts that needed interventions during the observation period to maintain patency. Data was analyzed using the Graphpad Prism Software (Version 8.0 for Mac, GraphPad Software, La Jolla California USA). The unpaired Student’s t test was applied to analyze normally distributed data. The Mann-Whitney-U-test was used when comparing data that was not normally distributed. Patency rates were estimated using the Kaplan-Meier method with Log-Rank test. A p<0.05 was considered to be statistically significant. A linear regression was used to visualize the number of interventions during the months the graft was in use for each individual graft. The study was approved by the Ethics Committee, Ethikkommission Nordwest- und Zentralschweiz (Project ID: 2018-00322).
3. RESULTS
A total of 12 patients with an acuseal and 13 patients with an ePTFE vascular graft were included in the study. The two groups did not differ with regards to age, gender, time on hemodialysis and observation time. The mean age of the study population was 63.5 years in the acuseal, 67.5 years in the ePTFE group. 58% of the patients in the acuseal and 46% of the patients in the ePTFE group were male. On the day of graft implantation patients had been on hemodialysis for 51.3 months in the acuseal and 60.5 months in the ePTFE group on average. The mean observation time was 280.5 days in the acuseal and 384.7 in the ePTFE group. There were three deaths in the acuseal, and five deaths in the ePTFE group. None of the deaths were related to graft complications.
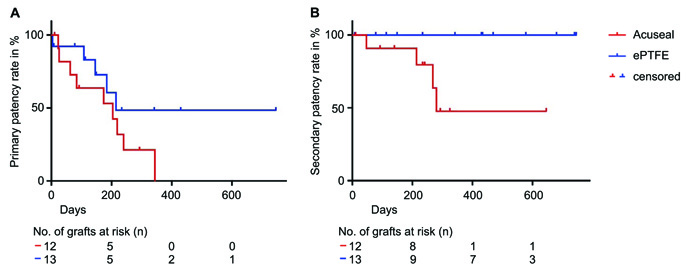
There was no difference in the time to the first intervention between the groups (153 days in the acuseal and 131 days in the ePTFE group; p = 0.70). Also the primary patency rate at the end of the observation period did not differ significantly between the acuseal and the ePTFE group (p = 0.16), (Fig. 1). With 48% in the acuseal and 100% in the ePTFE group the secondary patency rate at the end of the observation period was significantly worse in the acuseal group (p = 0.02), (Fig. 1). After the first intervention four of the acuseal vascular grafts were lost due to recurrent thrombosis despite several reinterventions (after a mean of 202 days). In the ePTFE group all the grafts could be used until the end of the observation period. The time from the first intervention until the end of the observation period was with 113 days significantly shorter in the acuseal group as compared to 449 days in the ePTFE group (p = 0.0002).
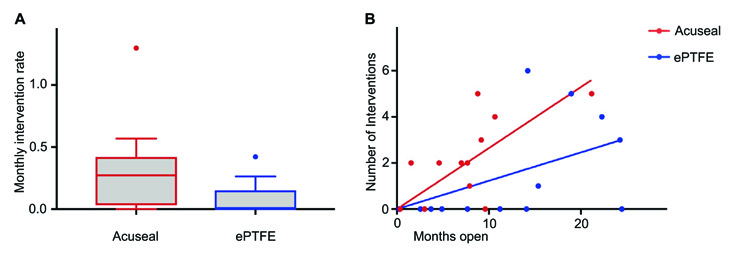
The monthly intervention rate per graft was significantly higher in the acuseal group with on average 0.33 interventions per month needed to maintain patency as compared to 0.08 interventions per month in the ePTFE group (p = 0.02, Fig. 2A). The number of interventions needed in each individual graft during the months the graft was in use is visualized in Fig. 2B (p = 0.02). In total 14 percutaneous transluminal angioplasties (PTAs) and 12 surgical interventions were performed in the acuseal group, 14 PTAs and five surgical interventions in the ePTFE group. There was no significant difference in the number of PTA or surgical interventions between the groups. The decision, whether a PTA or a surgical intervention was performed was taken in a joint conference by the attending vascular surgeon, angiologists and nephrologist depending on the vascular access properties, previous interventions, patient comorbidities and resources available.
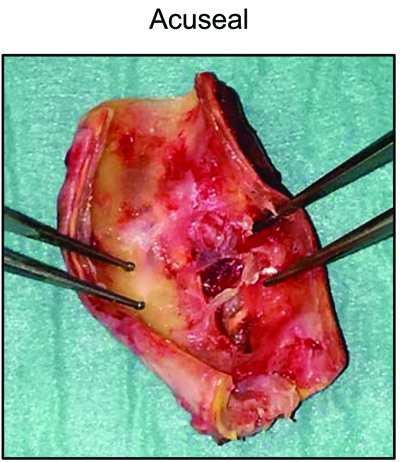
An example of an acuseal graft which had to be removed because of acute thrombosis is shown in Fig. (3). The depicted part of the acuseal graft has never been cannulated for hemodialysis.
4. DISCUSSION
Previously reported patency rates for acuseal vascular grafts differ widely [4]. Tozzi et al. reported primary and secondary 12 month patency rates of 68% and 93.3% respectively, whereas Aitken et al. observed a primary patency rate of 32% and a secondary patency rate of 40% at 12 month after implantation of the acuseal graft [5, 6]. Glickmann et al. conducted the largest prospective trial so far (138 patients receiving acuseal grafts) and reported a primary patency rate of 35% and a secondary patency rate of 79% [7]. A recent Meta-Analysis reported a twelve-month pooled primary and a secondary patency of 43.6% and 70.5% respectively [8].
In our study the primary patency rate was lower than expected from the literature, but comparable between the graft materials. Given the relatively low patient number of the present study, the acuseal primary patency rate could in theory be as high as 25%, since three patients with acuseal grafts were censored during the first year without needing interventions (two patients died, one only had an observation time of 293 days). In the present study, ePTFE vascular grafts, showed a significantly better secondary patency rate when compared to acuseal vascular grafts with fewer interventions needed to maintain patency. Surprisingly all ePTFE grafts could be rescued by interventions, whereas a high number of acuseal grafts needed reinterventions and four acuseal grafts were finally lost within the study period. One could argue that acuseal vascular grafts were preferentially implanted in patients who urgently needed hemodialysis. Uremia, hypotension and inflammation – all clinical characteristic of a patient in need of an unplanned dialysis start – could promote shunt thrombosis and negatively affect patency. Our data, however, argue against the influence of these factors, since the time to the first intervention was similar in both groups.
Studies comparing heparin-bonded ePTFE grafts without the tri-layer structure that is characteristic for acuseal vascular grafts with standard ePTFE grafts have yielded controversial results. Davidson et al. showed higher patency rates for heparin-bonded ePTFE grafts, whereas others observed no significant difference in patency rates between these groups [9, 10]. In a retrospective analysis Zea et al. showed higher reintervention and thrombectomy rates in patients with heparin-bonded ePTFE grafts when compared to patients with standard ePTFE grafts while patency rates did not differ between the groups [11]. The cause of the increased number of interventions needed in heparin-bonded ePTFE or acuseal vascular grafts remains to be determined. The aspect of an explanted acuseal vascular graft (Fig. 3) might suggest that the inner layer was damaged during earlier interventions, thus forming a more thrombogenic surface, inducing a higher number of needed reinterventions and ultimately leading to graft loss. The significantly shorter time from the first intervention until the end of the observation time in the acuseal group in comparison with the ePTFE group argues in favor of this concept.
There are several limitations to our study. It is a single center, non-randomized, retrospective, observational case series, which makes our data prone to bias. Due to the retrospective nature of the study there may be an inherent bias as to which patients received an acuseal or an ePTFE vascular graft and also surgeon`s preference may have biased the results. Probably the biggest limitation is the small sample size and the high variability in observation time. It is still remarkable though that a significant difference was detectable, indicative of a large effect of the graft type on intervention rate. This finding was consistent with our clinical perception.
CONCLUSION
Our data suggest that acuseal vascular grafts show a lower secondary patency rate when compared to ePTFE vascular grafts with more interventions needed to maintain patency. Larger studies comparing early cannulation grafts with ePTFE grafts with a particular focus on the outcome after the first intervention are needed to confirm our results.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study was approved by the Ethics Committee Ethikkommission Nordwest- und Zentralschweiz (Project ID: 2018-00322).
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
AVAILABILITY OF DATA AND MATERIAL
The authors confirm that the data supporting the findings of this research are available within the article.
FUNDING
The work was supported by a grant of the Fundação Pesquisa e Desenvolvimento Humanitario and the grant number is F- 85202-04-01.
CONSENT FOR PUBLICATION
Written consent has been waived in the decision of the ethical comity (Project ID: 2018-00322). All patients were informed about the study. All authors gave consent to publish the study.
CONFLICT OF INTEREST
Stephan Segerer receives financial support and travel expenses as a Speaker from Baxter and Fresenius. He is medical advisor for Peripal and Versantis. These are not related to the current study.
ACKNOWLEDGEMENTS
Declared none.

