All published articles of this journal are available on ScienceDirect.

Successful Reconstruction of the Penile Skin Loss Using a Scrotal Flap as a Result of Complete Resection Following a Traditional Circumcision: A Case Report
Authors Info & Affiliations
Abstract
Background:
Circumcision is the oldest and most common surgical procedure in the world. One out of three adult males is subjected to this procedure at some point in their lives. Circumcision is done for different reasons, most often to meet religious and/or cultural obligations. Though rare, there exist medical indications for this procedure. As in all surgical procedures, there are early or late complications or morbidities associated with circumcision ranging from mild to severe. The factors that influence the rate of occurrence of complications include: the surgical technique applied, the degree of asepsis during the procedure, and the expertise of the practitioner carrying out the procedure.
Case Presentation:
This is the case of a 20-year-old black male. He presented in the emergency department of the Douala Laquintinie Hospital (DLH) two hours after circumcision with persistent bleeding from the penile wound. This was performed by a traditional healer using the technique of guillotine. Examination of the external genitalia revealed a wound on the penis with loss of skin over the whole penile shaft. Under spinal anesthesia, a reconstruction intervention which involved a single step scrotal skin flap advancement over the penile shaft was done. We noted satisfactory healing process with a pleasing aesthetic appearance of the penis. He confirmed satisfactory penile erection and sexual activity two months after hospital discharge.
Conclusion:
Circumcision is a simple surgical procedure that can result to life threatening complications or high morbidity more often when performed by an unskilled practitioner. Education of the population on the safer sites of circumcision can help in the prevention and early management of complications.
1. BACKGROUND
Circumcision is a process that involves the surgical removal of the foreskin [1]. Worldwide, the overall prevalence of circumcision is estimated at 36.7% [2]. In Cameroon, up to 94% [3] of the male population is circumcised. Most often, this is done under religious and/or cultural obligations. During adolescence, circumcision is considered in some cultures as a rite of transition into adulthood [4, 5]. The benefits of circumcision in medical science is highly debatable in several countries [1]. Medically, circumcision has shown a benefit in reducing urinary tract infection in children [6], in reducing HIV infections by about 50 to 60% [7, 8], herpes simplex virus type 2 (HSV-2) infections [9], and Human Papillomavirus (HPV) High risk [10, 11] in the male sexually active adult population. Other studies have also shown the reduction of sexually transmitted infections, including HPV and trichomonas vaginalis infections among female partners of men who were circumcised [12-14]. Like all surgical procedures, circumcision can be associated with the number of minor to severe complications that can be life-threatening such as massive hemorrhage or sepsis [15, 16]. Weiss [17] in a systematic review performed in 2010 reports a median of 1.5% (0-16%) as a rate of minor complications and a median of 0% (0-2%) of major complications following a circumcision [17]. The most frequent are pain, bleeding, glans edema, excessive penile skin loss, strictures of the urethral meatus, the formation of a fibrous ring covering the glans, amputations of the glans and uretro cutaneous fistulas [17]. The surgical technique used, asepsis, traditional practitioner carrying out circumcision [17, 18] and even paramedical personnel [17] are factors in the occurrence of severe complications.
We report a case of successful reconstruction of the penile skin loss using a scrotal flap as a result of a complete resection by a traditional healer.
2. CASE PRESENTATION
This is the case of a 20-year-old black male. He presented in the emergency department of Douala Laquintinie Hospital (DLH) two hours after circumcision with persistent bleeding from the circumcision site. This was done by a traditional healer using the technique of the guillotine. The patient had no history of chronic conditions, and never described abnormal and persistent bleeding following any wound. He has never undergone any surgical intervention.
During clinical examination, he was conscious and alert. His vital signs were a blood pressure of 134/86 mmHg, heart rate of 88 beats per minute, a respiratory rate of 19 cycles per minute and a temperature of 37.6°C. Examination of the external genitalia showed a wound on the penis with loss of skin over the whole penile shaft Fig. (1). There was no more active bleeding. There were no abnormalities of the glans and the urethral meatus. The rest of the examination was unremark-able, with no signs of circulatory shock.
At the end of the clinical examination, we made the diag-nosis of accident on circumcision achieving minor bleeding associated with complete denudation of the penile shaft. It was therefore a delayed emergency indication to surgery. With regard to pre-operative work-up, the hemoglobin level was 12.2 g/dl, a platelet count of 245 109 /l. The rest of the examinations were unremarkable. Initial management consisted of the administration of analgesics, antibiotics, and tetanus immunoglobulin.
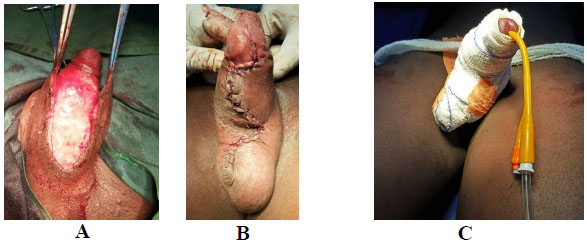
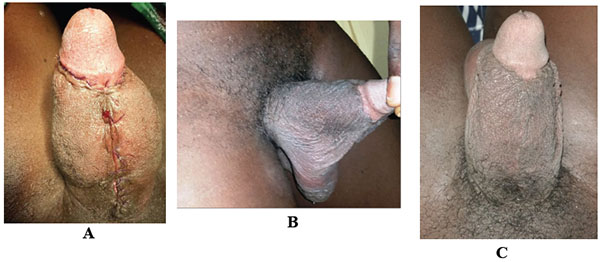
Twelve hours after admission, the patient underwent surgery under spinal anesthesia. He was installed supine; we achieved asepsis followed by sterile field placement. Subsequently, we found absence of hair on the scrotal skin, so we opted for a single step scrotal advancement flap. The main operating steps were: Skin incision on the scrotal median raphe; subcutaneous dissection of the scrotal skin on both sides of the median raphe respecting the vascular pedicles (posterior and anterior scrotal arteries). Subsequently, we realized a detachment of the scrotal skin while respecting the tunica vaginalis; followed by mobilization of the scrotal flap. This last was advanced gently over the penile and covering the penile shaft Fig. (2a). The sutures were made with absorbable Poly-glactin 3/0 thread by separate points Fig. (2b). A transurethral urinary catheter was placed and the bandage of the operative wound made Fig. (2c). Analgesic was continued postoperatively, as were as the antibiotics; Amoxicillin-clavulanic acid received for 5 days. The evolution in the postoperative period was marked by the occurrence of several episodes of spontaneous painful erection, which resolves spontaneously and of variable duration (30 to 45 minutes). The patient has benefited from anti androgenic: Cyproterone Acetate and a muscle relaxant with favorable evolution. A good evolution of the operative wound was noted Fig. (3). The discharge from the hospital was made on the 19th day after surgery, he had no more painful erections and the wound healing was complete. During the outpatient follow-up the patient reports a resumption of sexual activities 2 months after surgery with satisfactory erection and a satisfactory aesthetic appearance of the penis.

3. DISCUSSION
It was a case of circumcision performed in a 20-year-old adult by a traditional healer with the complication of a complete denudation of the penile shaft that required plastic reconstruction with a scrotal advancement flap. Circumcision is the most common surgical procedure in the world [1, 19] and one of the oldest interventions described. One out of three adult males is subjected to this procedure at some point in their lives [2]. Like all surgical procedures, complications are common, they can reach 50% in some series [15, 17]. Unskilled practitioner, poor preparation and poor technique are the factors involved in the occurrence of complications that may affect the functional and vital prognosis in case of major sepsis or massive bleeding [17].
As major complications, infections and urethral fistulas are the most common [18, 20] followed by hemorrhages, skin bridges and stenosis of the urethral meatus. Denudation of the penile shaft as a complication is relatively uncommon. Sylla and Diabate [18, 20] report respectively a frequency of 1 and 3% while Okeke report a frequency of 16% [16]. Several mechanisms may explain skin loss in the penile region following a circumcision. It can occur after direct excision during the major surgical procedure or following a postoperative skin infection or during postoperative debridement indicated for skin necrosis [21]. This loss of substance exposes the penis with subsequent major risk of infection and erectile dysfunction [19].
Several reconstruction techniques are possible, they are functions of the extent of the loss of substance, ranging from directed healing to skin grafts using thin or thick flaps [21]; fasciocutaneous advancement flap using a flap from the inguinal, femoral [22] and even scrotal region. In the case presented, the authors opted for a skin advancement flap using the scrotal skin. The mobilization of the scrotal flap during surgery was done respecting the vascularization of the tissues. Early post-operative care aimed to ensure proper flap healing while avoiding infections. The patient received frequent dressings with the use of normal saline. The frequent occurrence of spontaneous painful erections initially in the morning and then daily, motivated the administration of anti-androgens for the control of erections to allow proper healing tension-free. With regard to the resumption of sexual activity, there was no consensus on the duration of abstinence. In our case, sexual relations were allowed after complete healing of the penis and amendment of spontaneous painful erections.
In our context, traditions, lack of legal regulation as to the qualification required for this surgical procedure, the low cost of surgery proposed by the paramedical personnel expose low-income populations to go out of specialized centers to undergo circumcision. The prevention will start by the sensitization of the population and the training of all the persons implied in the practice of circumcision: traditional practitioner, paramedical personnel, medical doctors, and surgeons.
CONCLUSION
Circumcision is a simple surgical procedure and safe when performed by qualified personnel under strict aseptic conditions. Beliefs and traditions which are deeply rooted in mentalities, favor the rise to the malpractice of circumcision by traditional ways.
In cases of large penile skin loss, scrotal advancement flap remains a good option. It has many advantages in terms of aesthetic scar, functional skin and short hospital stay.
LIST OF ABBREVIATIONS
| DLH | = Douala Laquintinie Hospital |
| dl | = deciliter |
| g | = gram |
| HIV | = Human Immunodeficiency Virus |
| HPV | = Human Papillomavirus |
| HSV | = Human Simplex Virus |
| l | = liter |
| mmHg | = millimeter of mercury |
AUTHORS' CONTRIBUTIONS
NM and TWL, contributed in design of the study and writing of the manuscript.
ST, DG, KG, AF, contributed in critical reading.
NW, collected the pictures, and obtained the patient’s consent.
All authors have read and approved the final version of the manuscript.
ETHICS APPROVAL AND CONSENT TO PARTI-CIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
No animals were used in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
AVAILABILITY OF DATA AND MATERIAL
Not applicable.
FUNDING
None.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The authors would like to thank all the clinicians and staff of the Douala Laquintinie Hospital for the care of the patient.

