All published articles of this journal are available on ScienceDirect.

Parameters of Chronic Kidney Disease to Identify Outpatients at Increased Risk for COVID-19 Mortality: A Cohort Study of UK Biobank Participants
Authors Info & Affiliations
DEAR EDITOR,
Coronavirus Disease (COVID-19) has resulted in a pandemic affecting more than a hundred countries worldwide [1]. Limited worldwide supply of vaccines against severe acute respiratory syndrome coronavirus 2 (SARS-CoV) requires policymakers to prioritize high-risk populations for inoculation. Several clinical risk factors have been suggested to increase infection risk [2]. However, it is less well-known how pre-morbid, outpatient clinical variables influence COVID-19 risk of death. We retrospectively analyzed outpatient risk factors for death in the UK Biobank (UKBB), a large-scale prospective cohort comprising over 500,000 subjects aged 40-69 years recruited in 2006-2019 [3]. In this study, subjects with recorded mortality before 31st January 2020 (N = 28,930) were excluded since it was the date for the first recorded COVID-19 case in the UK. We performed a comprehensive study on primary care data and their associations with COVID-19 mortality in UKBB, controlling for possible confounding factors. To our knowledge, this is the broadest analysis of outpatient clinical factors and associations with COVID-19 to date.
COVID-19 outcome data were downloaded from the UKBB data portal on 23rd February 2021. Clinical Events were obtained from the Primary Care data for COVID-19 research in UKBB. In UKBB, we set a time window of 5 years before death with COVID-19 to identify active medical diagnoses that may be risk factors with COVID-19 death. The estimated glomerular filtration rate (eGFR) was calculated by the UKBB using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula, and urinary albumin to creatinine ratio (UAlb/UCr) was collected from UKBB. The diagnosis of COVID-19 was confirmed with at least one positive real-time reverse transcriptasepolymerase chain reaction (RT-PCR) test result in cases admitted with symptoms, signs, and findings (laboratory) suggestive of COVID-19. Patients without any RT-PCR positivity, and those considered as ‘possible’ or ‘probable’ cases according to the Center for Disease Control and Prevention (CDC) criteria, were not included in this study. Among 397,000 subjects in the UKBB with available GP clinical data and history of risk factors, 14,877 patients tested positive for COVID-19, and 1,994 of these patients had all the above risk factors and GP data available. We dropped most features that had more than 10% missing values resulting in 98 features. A subset of these 98 features is explained in Table 1 below.
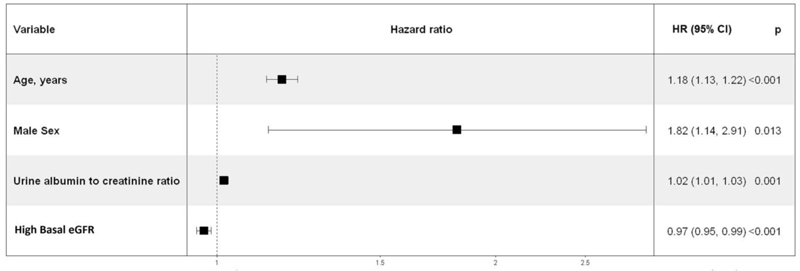
We performed multivariable-adjusted penalized Cox proportional hazards analysis on all features, including basic demographic variables (age, sex, ethnic group), comorbidities (coronary artery disease, diabetes, hypertension, asthma, COPD, depression, dementia, history of cancer), blood measurements (e.g., blood urea and creatinine reflecting renal function), indicators of general health (number of medications taken, number of non-cancer illnesses), anthropometric measures (body mass index BMI), socioeconomic status (Townsend Deprivation index) and lifestyle risk factor (smoking and alcohol disorder status). We then completed 10-fold stratified cross-validation and chose the model with the best coefficients to determine an optimal subset of features to use as predictors. Forest plots of the Cox proportional hazards regression model [4] for increased mortality in COVID-19 are shown in Fig. (1) below. Among 1,994 participants with COVID-19, the average age was 53.5 years with a standard deviation (SD) of 8.7, and 1,025 (51%) were male. The mortality rate was 4.1%. Multivariable Cox regression results showed that older age and male gender were significantly associated with death, consistent with prior studies [5]. Compared with female participants, male participants had a significantly higher risk of death (hazard ratio (HR) 1.82, 95% confidence interval (CI): 1.14 to 2.91, p=0.013). Importantly, our analysis revealed an association of baseline renal function with the risk of COVID-19-associated mortality. Improved eGFR was associated with a lower risk of death in individuals with COVID-19. Each 1 mL/min/1.73m higher eGFR was associated with a 3% lower risk of death (95% CI: 1% to 5% lower, p<0.001). Higher UAlb/UCr (HR 1.02, 95% CI: 1.01 to 1.03, p=0.001) was also significantly associated with death (Fig. 1).
| S.No | Clinical Characteristics | Overall Cohort (n=1994) |
Survived (n=1913) |
Dead (n=81) |
|---|---|---|---|---|
| 1. | Age, years | 53.52 +/- 8.72 | 53.08 +/- 8.58 | 63.75 +/- 4.84 |
| 2. | Sex (Female) (%) | 49 | ||
| 3. | Body mass index, kg/m2 | 28.65 +/- 3.48 | ||
| 4. | Ethnic background – White (%) | n= 614 (30.79%) | n=593 (30.99%) | n=21 (25.92%) |
| 5. | Ethnic background – Asian (%) | n= 299 (14.99%) | n=296 (15 47%) | n=3 (3.70%) |
| 6. | Ethnic background – Black (%) | n= 139 (6.97%) | n=137 (7.16%) | n=2 (2.46%) |
| 7. | Ethnic background – Unknown (%) | n= 942 (47.24%) | n=887 (46.36%) | n=55 (67.90%) |
| 8. | Coronary artery disease, n (%) | n=59 (2.96%) | n=56 (2.92%) | n=3 (3.70%) |
| 9. | Diabetes, n (%) | n=159 (7.97%) | n=152 (7.94%) | n=7 (8.64%) |
| 10. | Hypertension, n (%) | n=139 (6.97%) | n=135 (7.05%) | n=4 (4.93%) |
| 11. | Asthma, n (%) | n=119 (5.97%) | n=117 (6.11%) | n=2 (2.46%) |
| 12. | COPD, n (%) | n=37 (1.85%) | n=35 (94.59%) | n=2 (2.46%) |
| 13. | Depression, n (%) | n=19 (0.95%) | n=19 (1.82%) | n=0 (0%) |
| 14. | Dementia, n (%) | n= 26 (1.30%) | n=24 (1.25%) | n=2 (2.46%) |
| 15. | History of cancer, n (%) | n=173 (8.68%) | n=168 (8.78%) | n=5 (6.17%) |
| 16. | Systolic blood pressure, mmHg | 129.53 +/- 13.02 | 127.49 +/- 12.91 | 136.24 +/- 19.71 |
| 17. | Diastolic blood pressure, mmHg | 77.90 +/- 7.65 | 77.97 +/- 7.51 | 86.38 +/- 17.11 |
| 18. | Lymphocyte count, 10^9/L | 2.16 +/- 3.09 | 2.16 +/- 3.15 | 0.91 +/- 1.13 |
| 19. | Platelet count, 10^9/L | 254.68 +/- 46.02 | 255.02 +/- 44.62 | 215.34 +/- 25.65 |
| 20. | Urine albumin/creatinine ratio mcg/mg | 3.91 +/- 2.85 | 3.59 +/- 1.79 | 3.73 +/- 4.94 |
| 21. | 21. Urine creatinine, mg/dL | 0.86 +/- 0.17 | 0.85 +/- 1.65 | 0.24 +/- 1.78 |
| 22. | Serum blood urea nitrogen, mmol/L | 4.93 +/- 1.63 | 4.17 +/- 1.30 | 4.92 +/- 1.64 |
| 23. | Serum C reactive protein level, mg/L | 6.46 +/- 1.72 | 6.43 +/- 5.68 | 15.72 +/- 3.71 |
| 24. | Estimated glomerular filtration rate using chronic kidney disease epidemiology equation, mL/min/1.73m |
66.29 +/- 6.44 | 76.47 +/- 5.91 | 52.10 +/- 13.37 |
COVID-19 presents an unprecedented challenge due to its complex transmission patterns and our limited understanding of risk factors associated with mortality. The acute illness may confound hospital-specific variables to understand underlying susceptibility to infection and subsequent death. This study evaluated clinical risk factors before the hospitalization that were routinely collected as part of the participant’s primary care. We were able to leverage the outpatient data from the UKBB to understand underlying risk factors that could influence a patient’s risk for death with COVID-19. We found statistically and clinically significant associations between mortality in COVID-19 and baseline demographics and underlying kidney function. We found that death disproportionately affected older male patients. In addition, low eGFR and high UAlb/UCr were prognostic for mortality in COVID-19. We recommend that outpatients with a history of underlying kidney issues be monitored as high-risk for COVID-19 related complications. Furthermore, our findings suggest that COVID-19 vaccine administration should be prioritized for outpatients with a history of kidney complications.
Figure legend. We performed multivariable cox proportional analysis among 98 independent features to identify variables associated with the risk of death in COVID-19. The horizontal lines represent 95% confidence intervals, with arrows indicating extensions of the intervals. Boxes represent the point estimate.
CONSENT FOR PUBLICATION
Not applicable.
FUNDING
Funding was received from the NIDDK K23DK116967 (PB), Roche Diagnostics IIS (PB, WCL), NIH/NEI K23EY029246 (AL) and a career development award from Research to Prevent Blindness (AL).
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

