All published articles of this journal are available on ScienceDirect.

End-to-End Anastomotic Urethroplasty Outcome in Anterior and Posterior Traumatic Urethral Stricture: A Single-Center Experience
Authors Info & Affiliations
Abstract
Introduction
The objective of this study was to describe the results and associated factors of anterior and posterior traumatic urethral stricture after end-to-end anastomotic urethroplasty.
Methods
Medical records were used to retrieve clinical data. We included men over 18 years old who had a traumatic urethral stricture and were treated with end-to-end anastomotic urethroplasty. The data collection period was from January 2015 to December 2021, with at least 12 months follow-up period. After data screening, the data were divided into anterior and posterior strictures.
Results
Fifty patients were included in the study. The overall mean age was 42.06 (SD 12.4; 95% CI) years old, with a 21 (12-77) month median follow-up. %). The overall restricture rate was 36%. Furthermore, restricture rate in anterior stricture was 21.1%, while in posterior stricture was 45.2%. A significant association with restricture rate was found in the BMI category (p = 0.041) and etiology (p=0.03). There were 19 patients with anterior strictures and 31 patients with posterior strictures. Straddle injury was the most prevalent cause of anterior strictures (63.2%), whereas pelvic injury was the most common cause of posterior strictures (80.6%). For anterior and posterior groups, the majority of patients were normoweight (78.9% & 61.3%), entirely obliterated (63.2% & 64.5%), primary cases (84.2% & 80.6%), and done by reconstructive consultants (84.2% & 80.6%).
Conclusion
One-third of the patients experienced restricture arter end-to-end anastomotic urethroplasty, a higher restricture rate was found in posterior stricture. Restricture rate was associated with body mass index (BMI) and etiologies. End-to-end anastomotic urethroplasty may give durable patency if appropriately performed, especially in partial anterior traumatic urethral strictures.
1. INTRODUCTION
Traumatic urethral stricture is devastating long-term morbidity for men as it lowers the quality of life [1, 2]. In Indonesia, traumatic urethral stricture accounted for most cases of urethral stricture due to massive traffic accidents annually [3]. This is quite the opposite of industrialized countries where iatrogenic, due to instrumentation and catheterization, made a big proportion [1-4]. There are numerous surgical options for urethral stricture, but no particular procedure is ideal in every circumstance. Several factors, such as the length and location of the stricture, the condition of the fractured pubic bone segments, and the patient's age and general health, determine which surgical procedure to employ [5, 6]. There is ongoing controversy surrounding the selection between end-to-end anastomosis urethroplasty and free graft one-stage urethroplasty techniques. However, if appropriately indicated, end-to-end anastomotic urethro- plasty is anticipated to have a high long-term success rate, as no alternative is as effective as the urethra itself. Some evidence suggests performing end-to-end anastomotic urethroplasty in short anterior urethral stricture. To date, some authors also provide a promising patency rate in posterior strictures [7]. The outcome of end-to-end anastomotic urethroplasty is varied across studies, and very limited from the population of Southeast Asia. We conducted this study to describe the outcome of end-to-end anastomotic urethroplasty in anterior and posterior urethral stricture in our population.
2. MATERIALS AND METHODS
A retrospective study was conducted on all male adults (aged >18 years old) with traumatic urethral stricture who underwent end-to-end anastomotic urethroplasty from January 2015 to December 2021 at a national reference hospital in Indonesia (Fig. 1). All traumatic urethral strictures due to external trauma (straddle and pelvic injury) were included. Preoperative diagnosis was determined by retrograde urethrogram or bipolar urethro- cystogram through suprapubic cystostomy (SPC). Patients with incomplete data, iatrogenic-related strictures, and hypospadias were excluded. Patients with less than 12 months of follow-up were also exempted from the study. Approval from the institution's ethical research committee was obtained through approval number KET-70/UN2. F1/ETIK/PPM.00.02/2022 and protocol number 22-01- 0077. Written informed consent was obtained from patients before they underwent the surgery. A compre- hensive clinical evaluation was performed to define the strictures, including a thorough medical history and physical examination, uroflowmetry, and a retrograde urethrogram. After data screening, the data were divided into anterior and posterior strictures.
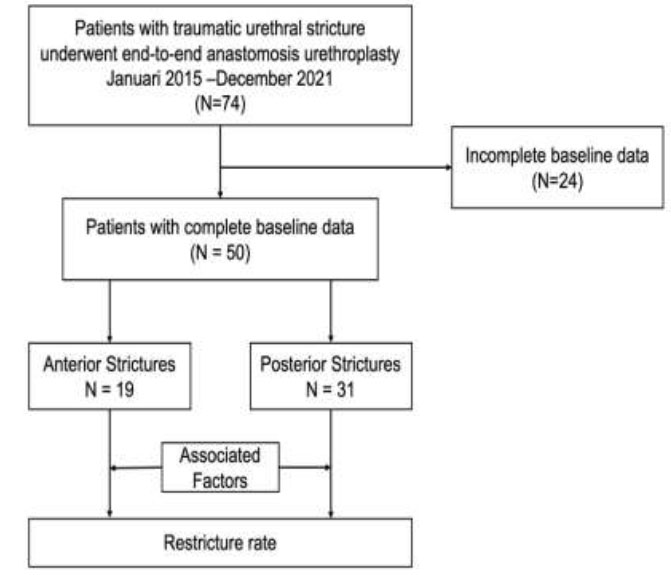
Flow of the studies.
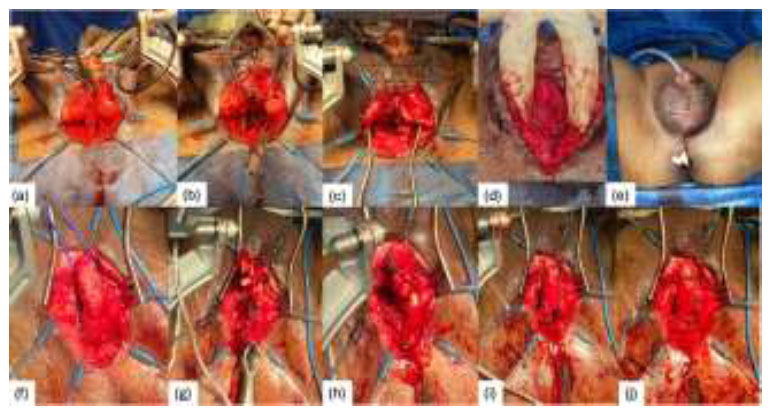
End-to-end anastomosis procedure in anterior urethral stricture (a-e) dan posterior urethral stricture (f-j). (a) urethral exposure after incision (b) pubectomy inferior (c) approximation of urethral ends (d) the anastomosis sutures (e) wound closure with Penrose drain. (f) mobilization of urethra (g) excision of fibrotic tissue and crural separation (h) approximation of urethral ends (i) anastomosis of urethral ends (j)anastomotic sutures.
2.1. Surgical Techniques
All of the patients in this study underwent standard procedure end-to-end anastomotic urethroplasty without graft for both anterior and posterior strictures. (Fig. 2) The procedure was performed in a lithotomy position and under general anesthesia. Urethroscopy was performed to evaluate the distal part of the stricture using 6 French urethroscopy. The first incision in the midline of the perineum to expose the bulbospongiosus muscle and corpus spongiosum. The urethra is mobilized and the corpus spongiosum is freed from surrounding tissue. A silicone Foley catheter was inserted through the orifice urethra until the obstructed part. The fibrotic tissue is excised until the healthy end. The distal punctum is approximated to the proximal healthy end. We must ensure tension-free approximation in this step, or particular maneuvers should be done. Surgical difficulties in posterior strictures escalate with each subsequent ancillary maneuver beyond urethral mobilization, which is performed sequentially to augment urethral mobility: from crural separation, partial pubectomy, supracrural rerouting to complete pubectomy and omental wrap. The urethral ends were spatulated and the anastomosis was performed using 3-0 absorbable sutures in six detached sutures. A Penrose drain is placed to close the surgical wound. Postoperative uroflowmetry and micturating urethrography were done one month after the procedure parallel with urethral catheter removal. SPC was removed 1-2 weeks later if the patient could void spontaneously.
2.2. Clinical Features
Anterior stricture comprised of bulbar stricture, while posterior stricture comprised membranous and prostatic stenosis. Restricture was defined as any postoperative instrumentation, including internal urethrotomy and redo urethroplasty. BMI was divided into normoweight (<23 kg/m2) and overweight/obesity (>23 kg/m2) based on the Asia-Pacific perspective WHO criteria for obesity. We divided the stricture length into short and long strictures with a cutoff of 20 millimeters, strictures length below 20 millimeters will be categorized as short strictures. Previous urethral dilation, internal urethrotomy, and urethroplasties were counted as previous urethral instrumentation. Primary cases included all patients who underwent urethroplasty for the first time. We contacted the patient through phone calls or surfing the admission history in medical records to obtain any complications such as erectile dysfunction, penile shortening, and incontinence. No objective diagnostic measurements were documented. The patient-reported outcome measure was not established during the period of data retrieval; thus, it was excluded from the parameters.
2.3. Statistical Analysis
All data was presented as a mean (standard deviation) if normal distribution was achieved, median (range) if normal distribution was not achieved, or percentage. All covariates, including the patient's age at surgery, body mass index (BMI), stricture obliteration, stricture length, previous urethral intervention (including internal urethrotomy and dilatation), previous urethroplasty, etiologies, surgery duration time, estimated blood loss, and complications during surgery, were investigated using univariate logistic regression. Statistical analysis was conducted using IBM SPSS Statistic version 25 for Mac. The significant P values were achieved when the value was below 0.05.
3. RESULTS
From January 2015 to December 2021, 74 male patients with traumatic urethral stricture underwent end-to-end anastomotic urethroplasty in our center. Of those patients, there were only 50 with completed baseline data included in the study. The overall mean age was 42.06 (SD 12.4; 95% CI) years old, with an overall median follow-up of 21(12-77) months. The overall median operating time was 180(80-360) minutes, while the overall median blood loss was 200(50-1300) mL. The demographics and clinical information of the cases were summarized in Table 1. The cases were mostly total obliteration (64%), primary cases (82%), caused by pelvic injury (64%), done without ancillary maneuvers (68%), and located in the posterior part of the urethra (62%). The overall restricture rate in our study was 36%. The majority of procedures were performed by a consultant, accounting for 84% of cases, whereas the reported rate of complications was 18%. A significant association with restricture rate was found in the BMI category (p = 0.041) and etiology (p=0.03). The included cases were then divided into anterior and posterior strictures. The characteristics of the anterior and posterior strictures were respectively described in Table 2. The anterior strictures comprised 19 patients with an overall restricture rate of 21.1%. The strictures were mostly short (73,7%), total obliteration (63,2%), and caused by straddle injury (63.2%). Of the 31 patients in the posterior strictures, the overall restricture rate (45.2%). The strictures were mostly long (54,8%), total obliteration (64,5%), and caused by pelvic injury (80,6%). The mean surgery time in anterior stricture was 135(80-290) minutes, while in posterior stricture was 180(100-360) minutes. Ancillary maneuver in the posterior strictures was done in 45.2%, while in the anterior strictures was only 10 percent. The restricture rate in redo end-to-end anastomotic urethroplasty was also higher in the posterior strictures (35.7% vs 25%). The reported complications from the patients were erectile dysfunction (2 patients), stress incontinence (2 patients), and penile shortening (1 patient).
| Variable |
N (%) (N= 50) |
Restricture Proportion |
P value# Odds Ratio |
|
|---|---|---|---|---|
| Age (years old) | - | 42.06 (12.4) | - | 0.789 |
| BMI (kg/m2) | - | 20.8(15.4-31.2) | - | 0.203 |
| BMI Categories | Normal | 34 (68%) | 26.4 | 0.041* |
| - | Overweight/ Obese |
16 (32%) | 56.3 | OR 3.6(1-12.4) |
| Stricture Length (mm) | - | 15(3-65) | - | 0.596 |
| Stricture Length Category | Short | 28 (56%) | 39.2 | 0.585 OR 0.72(0.2-2.3) |
| - | Long | 22 (44%) | 31.8 | |
| Operating Time (minutes) | - | 180(80-360) | - | 0.992 |
| Estimated Blood Loss (mL) | - | 200(50-1300) | - | 0.534 |
| Obliteration | Partial | 18 (36%) | 38.8 | 0.75 |
| - | Total | 32 (64%) | 34.3 | OR 0.8(0.25-2.7) |
| Etiology | Straddle | 18 (36%) | 16.7 | 0.03* |
| - | Pelvic Injury | 32 (64%) | 46.9 | OR 4.4(1-18.2) |
| Location | Anterior | 19 (38%) | 21 | 0.085 |
| - | Posterior | 31 (62%) | 45.1 | OR 3(0.8-11.4) |
| Operator | Consultant | 42 (84%) | 38 | 0.694 |
| - | Trainee | 8 (16%) | 25 | OR 0.5(0.1-3) |
| Previous Urethral Intervention | Yes | 14 (28%) | 50 | 0.198 OR 2.2(0.64-8) |
| - | No | 36 (72%) | 30.5 | |
| Primary Urethroplasty | Yes | 41(82%) | 31.7 | 0.253 OR 2.6(0.6-11.7) |
| - | No | 9 (18%) | 55 | |
| Restricture | Yes | 18 (36%) | - | - |
| - | No | 32 (64%) | - | - |
| Restricture in redo urethroplasty | Yes | 6 (33%) | - | - |
| - | No | 12 (67%) | - | - |
* statistically significant (P <0,05)
| Variable |
Anterior (N= 19) |
Restricture (%) |
Posterior (N=31) |
Restricture (%) |
|
|---|---|---|---|---|---|
| Age (years old) | - | 45(11.9) | - | 40.26(126) | - |
| BMI (kg/m2) | - | 21.2(17.9-41.2) | - | 20.7(15.4-27.5) | - |
| BMI | Normal | 15 (78.9%) | 3 (20%) | 19(61.3%) | 6 (31.6%) |
| - | Overweight/ Obese |
4 (21.1%) | 1 (25%) | 12(38.7%) | 4 (33.3%) |
| Stricture Length (mm) | - | 12 (3-30) | - | 20 (5-65) | - |
| Stricture Length Category | Short (<2 cm) | 14 (73.7%) | 4(28.4%) | 14 (45.2%) | 7 (50%) |
| Long (>=2 cm) | 5 (26.3%) | 0 (0%) | 17 (54.8%) | 7 (41.2%) | |
| Operating Time (minutes) | - | 135(80-290) | - | 180(100-360) | - |
| Estimated Blood Loss (mL) | - | 100 (50-1200) | - | 250 (50-1300) | - |
| Obliteration | Partial | 7 (36.8%) | 0(0%) | 11(35.5%) | 7 (63.6%) |
| - | Total | 12 (63.2%) | 4(33.3%) | 20(64.5%) | 7 (35%) |
| Etiology | Straddle Injury | 12 (63.2%) | 2 (16.7%) | 6(19.4%) | 1 (16.7%) |
| - | Pelvic Injury | 7 (36.8%) | 2 (28.6%) | 25(80.6%) | 13 (52%) |
| Operator | Consultant | 16 (84.2%) | - | 26(83.9%) | - |
| - | Trainee | 3 (15.8%) | - | 5(16.1%) | - |
| Previous Urethral Intervention | Yes | 5 (26.4%) | 2(40%) | 9(29%) | 5 (55.6%) |
| No | 14 (73.6%) | 2(14.3%) | 22(71%) | 9 (40.9%) | |
| Primary Urethroplasty | Yes | 16 (84.2%) | 2(12.5%) | 25(80.6%) | 11 (44%) |
| No | 3 (15.8%) | 2(67%) | 6(19.4%) | 3 (50%) | |
| Restricture | Yes | 4 (21.1%) | - | 14(45.2%) | - |
| - | No | 15 (78.9%) | - | 17 (54.8%) | - |
| Restricture in redo urethroplasty | Yes | 1 (25%) | - | 5(35.7%) | - |
| - | No | 3 (75%) | - | 9(64.3%) | - |
4. DISCUSSION
An ideal surgery of urethral stricture should remove the strictured urethra and reattach the ends without introducing foreign tissue. This is precisely what is accomplished with excision and primary anastomosis [7]. The constraint is influenced by the elasticity of the mobilized, healthy urethra after the stricture is removed. The elasticity of the anterior urethra is sufficient to allow for a 2-3 cm length span. While defects measuring 7-9 cm in length can be restored in the posterior urethra by employing ancillary maneuvers to achieve the desired tension-free anastomosis [8, 9]. Across studies, end-to-end anastomotic urethroplasty is considered a preferred therapeutic option for small strictures, particularly those located in the anterior (bulbar) region. However, this procedure is unsuitable for pendulous stricture because it may induce excessive shortening and ventral curvature of the penis. Our study showed an overall restricture rate in traumatic urethral stricture of 36%, significantly associated with etiology and BMI (p<0.05). The success rate was comparable to other studies. Furthermore, we describe the outcome of anterior and posterior strictures after the procedure in traumatic urethral stricture patients.
Our study demonstrated the restricture rate is quite high in the posterior urethral stricture. The lower success rate in posterior stricture was associated with many related factors. The mechanism of trauma as etiology was thought to affect the restricture rate according to the complexity. The external trauma mechanism caused by pelvic injury disrupted the bulbomembranous junction. According to Casselman and Schillinger's theory, the urethra is injured in major pelvic fracture cases when the pelvic ring is compressed laterally, increasing the antero-posterior diameter, superior bladder displacement, and urethral stretching and avulsion follow [10]. A study by Fu et al. [11] also showed that strictures closer than 3 cm to the bladder neck were predictors of poor prognosis. These kinds of strictures frequently necessitate more complicated surgery and carry a greater chance of failure. However, our results showed that the restricture rate of end-to-end anastomotic after redo urethroplasty is similar between the anterior and posterior strictures. As scarring and low tissue vascularity, recurrent urethral strictures provide surgical difficulties [12].
We found no significant association between age and restricture rate. However, Davenport et al. [13] reported that men under 40 had better outcomes after urethroplasty than older men because they had fewer comorbidities predisposing them to impaired vascularity and tissue healing than older men. Testosterone level was also believed to be related to restricture in older age. After age 30, testosterone levels begin to decline at a rate of 0.4% to 2% per year [14-16]. Men with reduced amounts of testosterone in their bloodstream may experience a decline in the blood vessel density inside the urethral and corpus spongiosum tissue. This can be attributed to a drop in the expression of AR (androgen receptor) and TIE-2, a receptor for angiopoietin 1 and involved in angiogenesis mediated by AR. In contrast, studies conducted by Barbagli et al. [17] and Santucci et al. [18] revealed comparable outcomes for younger and geriatric patients. Therefore, the success rate of end-to-end anastomotic bulbar urethroplasty is not solely influenced by patient age and should not be considered when making decisions on the implementation of these procedures.17,18 Although older men are more likely to have multiple comorbidities, their eligibility for urethroplasty should be based on their overall health, not their age [19].
In our study, BMI is a significant factor in restricture occurence. A Cut-off of 23 kg/m2 was used based on the WHO classification for the Asia Pacific population. A higher restricture rate was associated with higher BMI. This result was consistent with a prior investigation by Breyer and colleagues [20]. They found the patients with overweight (25-30 kg/m2) and (30-35 kg/m2) BMI were more likely to experience stricture recurrence than those with a normal BMI between 0-25 kg/m2 and individuals with a BMI of 35 kg/m2 or greater. The precise mechanism by which obesity increases the risk of postoperative complications is unknown and probably multifactorial [21]. Several studies have demonstrated plausible mechanisms, including low-grade inflammation, impaired collagen regeneration, and vascular insuffi- ciency. Inflammation is essential for the development of urethral stricture [22]. In addition, obesity is associated with impaired immune function, which may contribute to the higher incidence of surgical site infections observed in obese patients [23]. According to a study conducted by Elliott et al. [24], both obesity and age were significant determinants of the treatment for urethral stricture. There is debate about whether greater stricture rates in obese individuals are a result of technical problems or whether obesity has an influence on wound healing [25]. Posterior urethral surgery necessitates a high level of expertise and a thorough understanding of the relevant organs' specific anatomical and functional attributes beyond that required in any other segment of the urethra [26].
In our study, there was no correlation between previous urethral instrumentation and the incidence of restricture. There were contradictory findings regarding the impact of prior urethral instrumentation, such as internal urethrotomy, on the efficacy of urethroplasty. According to Roehrborn et al. [27], prior urethral intervention reduces the efficacy of end-to-end anas- tomotic urethroplasty. Similar to this result, Breyer et al. [28] determined that endoscopic treatment failure was a predictor of urethroplasty failure. It is hypothesized that previous DVIU for traumatic posterior urethral injuries will extend the inflammatory process along the already injured tissue, making urethroplasty difficult in the future.19,28 Nonetheless, according to a study by Barbagli et al.17, the prior failure of urethrotomy does not affect the long-term efficacy of bulbar urethroplasty.
Table 2 shows restricture rate is lower in the long anterior group . However, this might be due to a discrepancy in the number of subjects in short and long stricture. Restricture rate in the posterior group is quite similar between short and long stricture. Due to the lengthier stricture length and more complex surrounding structures, ancillary maneuvers were performed more often in the posterior strictures in this study. Longer urethral defects in posterior strictures necessitate a complex perineo-abdominal transpubic approach for adequate exposure. Furthermore, pubic symphysis resection makes the tension between the anterior and posterior urethral anastomoses decrease significantly while the pelvic ring maintains its integrity [9].
Post-operative erectile dysfunction, penile shortening, and incontinence were common complications after urethroplasty. We reported a few cases of those complications based on documented data. The number should be higher as the patient-reported outcome was established in our hospital. However, those with complications did not get any further treatment as they were satisfied with spontaneous voiding. Penile shortening was reported to occur up to 30% in several studies, especially in anterior strictures. Post urethroplasty stress incontinence occurred in less than 10%. The incidence of erectile dysfunction following urethroplasty occurred up to 50% [7, 9]. It appears that the majority of men with erectile dysfunction have it as a result of the pelvic fracture itself. Cavernous nerves and branches of the internal pudendal artery are hypothesized to supply the corporeal bodies via the urogenital diaphragm and are situated in close proximity to the apex of the prostate. A pelvic fracture, specifically pubic symphysis diastasis, caused injury to these neurovascular bundles [9].
This research has several limitations. Due to inadequate documentation, we did not analyze long-term complications such as incontinence, erectile dysfunction, and penile shortening after the procedure. Postoperative uroflowmetry was unidentified in most patients, so the objective parameter was missing. Second, this retrospective study was conducted at a single facility and may not accurately represent the urethral stricture patient population or treatment patterns across the nation. Nonetheless, we accomplished our objective of describing the outcomes of anterior and posterior traumatic strictures after urethroplasty. A prospective, multi-institutional investigation would be useful for validating our findings. Due to inadequate documentation, our study only included a small number of samples; this could be a contributing factor to the insignificant associations. Due to the lack of evidence regarding the comparison of anterior and posterior urethral stricture outcomes, we provided only a general explanation of each factor.
Despite those limitations, our study is the first in Indonesia, a developing country with abundant traffic accidents, to describe the outcome of end-to-end anastomotic urethroplasty of traumatic urethral strictures with a moderately long follow-up period. Thus, a further multicenter prospective study on a large number of patients with multivariate analysis or a systematic review and meta-analysis across available studies is recom- mended to investigate the outcomes after end-to-end anastomotic urethroplasty.
CONCLUSION
The overall restricture rate after end-to-end anastomotic urethroplasty in traumatic urethral stricture was 36%, a higher restricture rate was found in posterior traumatic stricture. BMI and etiologies were associated with restricture occurrence. The present study may suggest end-to-end anastomotic urethroplasty to be performed in traumatic urethral strictures with potential durable patency if appropriately done. End-to-end anastomotic urethroplasty in partial anterior stricture in this study showed the lowest restricture occurrence.
AUTHORS’ CONTRIBUTION
It is hereby acknowledged that all authors have accepted responsibility for the manuscript's content and consented to its submission. They have meticulously reviewed all results and unanimously approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| SPC | = Suprapubic Cystostomy |
| BMI | = Body Mass Index |
| PFUD | = Pelvis Fracture Urethral Defect |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study obtained ethical approval from the Health Research Ethics Committee - Faculty of Medicine Universitas Indonesia and Dr. Cipto Mangunkusumo National Hospital (HREC FMUI-CMH), approval number KET-70/UN2.F1/ETIK/PPM.00.02/2022 and protocol number 22-01-0077.
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.

