All published articles of this journal are available on ScienceDirect.

NLR as a Predictive Factor for Prognosis after Varicocelectomy Surgery: A Systematic Review
Abstract
Introduction
Varicocele, characterized by abnormal dilation of the testicular veins, is a common condition affecting male fertility. The role of the neutrophil-to-lymphocyte ratio (NLR) as a predictive prognostic marker for varicocelectomy outcomes in improving male fertility remains uncertain. This systematic review aims to explore the association between pre-operative NLR levels and varicocele surgery outcomes.
Methods
A systematic literature search was performed following PRISMA guidelines, utilizing electronic databases such as PubMed, EMBASE, and Cochrane. Studies published between 2018 and 2024 were included if they examined varicocelectomy surgical outcomes and NLR levels as predictive factors. Data extraction and quality assessment were carried out independently.
Results
Four studies met the inclusion criteria, collectively involving 442 patients. Elevated NLR levels were associated with varicocele surgery failure, indicating the potential impact of inflammation on treatment efficacy. Pre-operative assessment of NLR levels showed promise in identifying candidates likely to benefit from varicocelectomy, thereby optimizing treatment outcomes. This is the first systematic review evaluating the prognostic utility of NLR in varicocelectomy outcomes. Elevated pre-operative NLR levels were associated with poorer surgical outcomes, highlighting their potential for pre-surgical patient stratification.
Discussion
The findings suggest that incorporating NLR into the pre-operative assessment of infertile men with varicocele could enhance treatment decision-making and improve overall fertility prospects. Elevated NLR levels were associated with varicocele surgery failure, suggesting the detrimental impact of inflammation on treatment efficacy.
Conclusion
Pre-operative assessment of NLR levels may aid in identifying candidates likely to benefit from varicocelectomy, optimizing treatment outcomes.
1. INTRODUCTION
A varicocele refers to an abnormal widening and twisting of the network of veins within the scrotum known as the pampiniform venous plexus. Typically, the left side is predominantly affected due to anatomical factors related to the internal spermatic vein (ISV). A prior investigation, utilizing femoral and spermatic venography, revealed that the ISV is exclusively implicated in both initial occurrences and recurrences of varicoceles [1]. Varicocele affects 15% of healthy males, 35% of those experiencing primary infertility, and up to 80% of those facing secondary infertility [2]. It has been widely accepted and established that during inflammatory responses, ROS provided by leukocytes or granulocytes have damaging effects on human spermatozoa, causing a marked loss of sperm motility and morphology and thus reducing hyperactivation and oocyte penetration [3]. Varicocele repair is a reasonable consideration as the primary treatment option when a couple with documented infertility involves a man with a palpable varicocele and suboptimal semen quality, and the female partner has a normal evaluation [4, 5].
Identifying predictive factors for the response to varicocelectomy is essential. Certain researchers argue that a higher grade of reflux in the testicular vein and a diameter exceeding 2.5 mm are associated with more substantial improvements in sperm parameters post-surgery [6, 7]. Conversely, other studies have found no significant enhancement in sperm parameters rates when assessing postoperative varicocele size [8, 9]. Likewise, while some researchers confirm that the absence of testicular atrophy predicts higher postoperative sperm parameters rates [6] others suggest that a smaller left testis size reduces the likelihood of improvement in fertility outcomes [10].
Although numerous studies have reported improvements in semen parameters after varicocele surgery, there are conflicting reports on its effectiveness, with some studies indicating that varicocelectomy may not be an effective treatment for male subfertility [5]. Therefore, it is crucial to identify which patients are likely to benefit from varicocelectomy. Consequently, numerous studies have attempted to determine the predictive value of various characteristics [11, 12].
Inflammatory conditions are well-recognized factors contributing to male infertility [13, 14]. It has been proposed that inflammatory processes also play a role in varicocele development. Certain inflammatory cytokines, found at high levels in men with varicocele, may activate neutrophils, influencing infertility and varicocele pathogenesis. Conversely, other cytokines may aid sperm motility by reducing inflammation [3, 15].
Various biochemical and hematological markers are utilized to assess systemic inflammation. Recently, the neutrophil-to-lymphocyte ratio (NLR) has gained popularity as a marker for cancer, systemic diseases, and inflammation [16-18]. Therefore, we aimed to explore pre-operation NLR as a factor that might predict the outcome of varicocelectomy surgery.
2. METHODS
2.1. Search Strategy
A systematic literature search adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines are shown [7]. The search was carried out on several electronic databases, such as PubMed, EMBASE, and Cochrane. Keywords and Medical Subject Headings (MeSH) terms related to “Varicocele,” “Neutrophile to Lymphocyte Ratio,” “Varicocelectomy,” “Predictor Factor,” and “prognosis” were used in the search strategy. Boolean operators (AND, OR) were employed to combine these terms appropriately. Only publications published in the English language between 2018 and 2024 were included in the search.
2.2. Selection Criteria
Inclusion criteria were defined to select relevant studies for the systematic review. Studies were included if they met the following criteria: 1) articles written in English language, 2) human participant studies, 3) full-text availability, 4) publication dates between 2018 and 2024, 5) study designs involving prospective, retrospective, cross-sectional, and case-control cohort studies, 6) studies examining varicocelectomy surgical outcomes, and 7) evaluations of NLR as predictive factors. The exclusion criteria include studies with irrelevant titles or abstracts, studies with unretrievable full texts, non-English studies, and studies categorized as case series, editorials, or review articles.
2.3. Data Extraction
Data extraction was conducted by two reviewers (SR and RP) working independently, and of there was any discrepancy, it was addressed through discussion between both the authors. Information about the studies (including authors and the year of publication), sample size, study results, specifications of diagnostic modalities utilized, and the sensitivity of those modalities were extracted from each included study. Specifically, data relevant to Varicocelectomy surgical outcomes, assessments of semen motility, and evaluations of NLR as predictive factors were meticulously extracted for analysis. Additionally, any data related to growth metrics was also captured.
3. RESULTS
3.1. Study Selection
A total of 28 studies were identified, none were duplicates. All identified studies underwent screening, resulting in the exclusion of 24 studies (Fig. 1). Four studies underwent full-text assessment, and all were included in this review. These papers were selected based on their alignment with the study's objectives and criteria outlined in the methods’ section [19-22]. All studies showed low-risk of bias (Fig. 2).
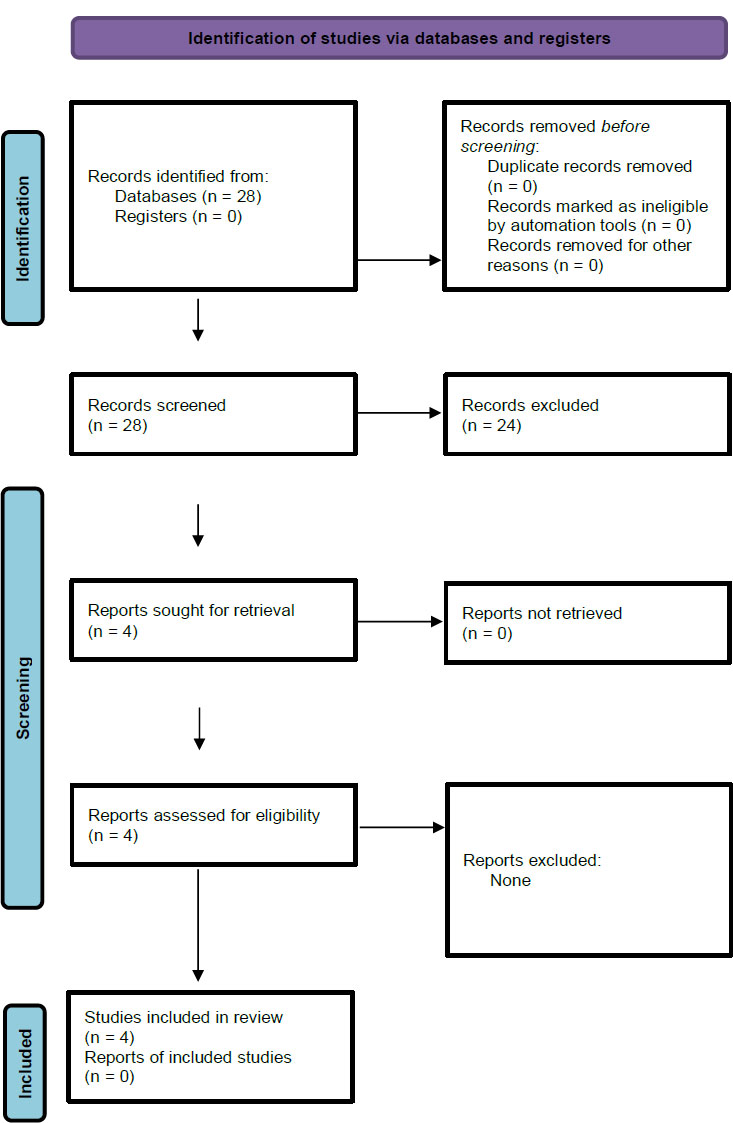
PRISMA flow diagram.
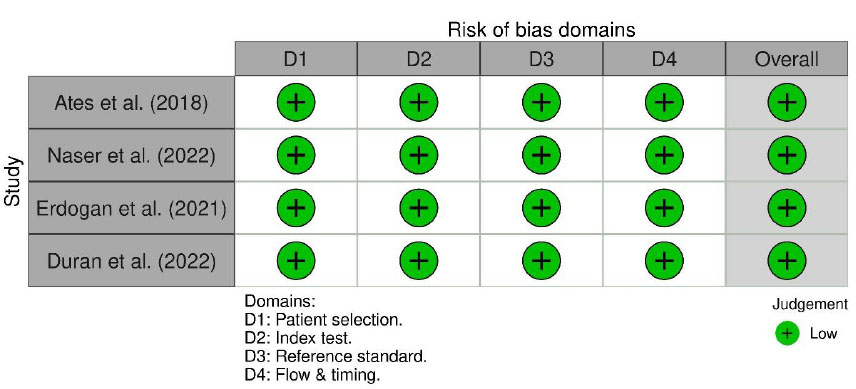
Risk of bias assessment using QUADAS-2.
3.2. Included Articles
According to research by Ates et al. [19], NLR is higher in the group as an independent predictor where varicocele surgery was unsuccessful (Table 1). These findings imply that inflammation might adversely affect the effectiveness of varicocelectomy. Kandevani et al. [20], found that laboratory hematology testing using NLR calculation could help plan the treatment for infertile men undergoing varicocelectomy. Semen analysis parameters can be improved in nearly all infertile males having varicocele with varicocelectomy. The efficacy of varicocelectomy for enhancing fertility and the suitable infertile candidates for varicocele surgery can be predicted and identified by using BMI, NLR, and baseline TMSC as the suggested scoring system. Omer et al. [21], found that infertile patients who benefit from microsurgical varicocelectomy tend to have a lower pre-operative neutrophil/lymphocyte ratio and a higher mean platelet volume (MPV). Therefore, a low neutrophil/lymphocyte ratio (≤2.27) and a high MPV ratio (≥9.45) are helpful pre-operative predictors for determining which infertile varicocele patients may benefit the most from varicocele surgery. Additionally, according to Duran et al. [22], low NLR and MLR prior to varicocelectomy were significant predictors of successful outcomes. Specifically, patients with lower values showed 2.9 and 2.5 times higher significant improvements when NLR <2.02 and MLR <0.22, respectively, when these values were taken into consideration as cut-off values.
3.3. Populations of Included Articles
The four included papers involved 442 patients and were published between 2018 and 2024. These studies provided valuable insights into Varicocelectomy surgical outcomes, semen analysis assessments, and NLR evaluations as prognostic predictors after varicocele surgery.
4. DISCUSSION
Varicocele is the most prevalent correctable medical condition leading to male infertility. The preferred and most effective treatment for varicocele is subinguinal microsurgical varicocelectomy [23]. Numerous studies have examined the beneficial impact of varicocelectomy on sperm parameters; however, a consensus has not been reached because of differences in inclusion criteria and variations in treatment methods across these studies [24-26]. As a result, several factors, including age, varicocele severity, pre-operative semen characteristics, reproductive hormones like FSH and testosterone, testicular size, testicular venous diameter, body mass index (BMI), and DNA fragmentation index, were assessed prior to varicocele surgery to determine the potential enhancement in semen parameters following the procedure.
This systematic review demonstrates that elevated preoperative neutrophil-to-lymphocyte ratio (NLR) is consistently associated with poorer outcomes after varicocelectomy. All four included studies found that patients with higher NLR values before surgery experienced significantly less improvement in postoperative semen parameters [19-22]. For instance, Ates et al., reported that the mean preoperative NLR was markedly higher in men whose varicocelectomy failed to improve fertility compared to those with successful outcomes [19]. Similarly, other groups observed that patients who benefited from varicocelectomy tended to have a lower NLR preoperatively [21, 22]. These findings underscore the potential of NLR as an informative prognostic marker: a low preoperative NLR may identify varicocele patients more likely to achieve favorable semen improvements after surgery, whereas an elevated NLR might flag those at risk of limited benefit. Incorporating NLR into pre-surgical evaluation could therefore enhance patient counseling and individualized decision-making, helping optimize fertility treatment plans [27, 28].
Table 1.
| Author | Year | Country | Design | Subject (n) | Mean/ Range Age | Varicocele Grade | Side | Mean/Median NLR in the Successful Group | Mean/Median in Unsuccessful Group | Outcome/Varicocelectomy Success Definition | NLR | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| AUC | 95% CL | p-value | Cutoff | Sensitivity | Specificity | PPV | NPV | |||||||||||
| Ates, et al. [19] | 2018 | Turkey | Retrospective cohort | 86 | 27.5 ± 4.9 | The subjects of this study consisted of patients with grade 1, 2, and 3 varicoceles. Mostly are grade 3. | 69 subjects have varicoceles on the left side, and 17 have bilateral varicoceles. | 1.7±0.3 | 2.3±0.5 | More than 50% increase in total motile sperm count in postoperative semen analysis was defined as a significant improvement. | 0.892 | 0.816-0.968 | <0.001 | ≤ 1.98 | 0.947 | 0.759 | N/A | N/A |
| Kandevani, et al. [20] | 2019 | Iran | Prospective cohort | 124 | 21.92±2.67 in success group and 22.66±3.16 in unsuccessful group | conducted on patients with varicocele of grade II or higher with mostly are grade 3. | 116 subjects have varicoceles on the left side and 8 subjects on the right side. | 1.68±0.68 | 2.28±0.43 | 6 months after the operation, semen analysis was repeated. Treatment success was defined as 50% increase in TMSC in cases with preoperative TMSC> 5 million/cc or a 100% increase in TMSC in cases with preoperative TMSC< 5 million/cc. | 0.808 | 0.716-0.899 | 0 | 1.8 | 87.5% (85.29-89.49%) | 76.9% (74.16-79.48%) | 79.11% (77.14-80.96%) | 86.02% (83.88-87.91%) |
| Omer, et al. [21] | 2021 | Turkey | Retrospective cohort | 130 | 29.1 years ±5.4. 29.5 ± 5.8 in success group and 28.4 ± 5.2 in unsuccessful group | The subjects of this study consisted of patients with grade 1, 2 and 3 varicoceles. Mostly are grade 3. | 117 subjects have varicoceles on the left side and 13 have bilateral varicoceles. | 1.84 (0.58) | 2.86 (1.2) | Success was defined as improvement of all semen parameters (concentration, progressive motility, and morphology) to normal values 6 months after surgery | 0.857 | 0.731 | <0.001 | ≤2.27 | 0.857 | 0.731 | N/A | N/A |
| Duran et al. [22] | 2022 | Turkey | Retrospective cohort | 102 | 28.6 ± 6.8 years | The subject consists of 12 patients Grade 1, 55 patients grade 2, and 35 patients with grade 3 varicocele. | 96 patients have | 1.4 ± 0.7 | 1.9 ± 0.8 | In this study, more than 50% increase in total motile sperm count on postoperative semen analysis was defined as a significant improvement. In addition to that, patients with a total motile sperm count of <5 million were also required to have an increase of >100% for indicating significant improvement. |
0.636 | 0.519–0.754 | 0.028 | < 2.02 | 0.875 | 0.4 | N/A | N/A |
Notably, our review is a qualitative synthesis rather than a meta-analysis. Given the small number of studies and heterogeneity in their design and outcome definitions, a formal meta-analytic pooling of data was not feasible. Instead, we compared results across studies. One area of heterogeneity defined what constitutes a “high” NLR. The optimal NLR cut-off values varied among the studies from approximately 1.8 to 2.3 [19-22]. For example, one study found that an NLR >1.98 best predicted failure to improve the total motile sperm count (TMSC) [19], while another identified a threshold NLR >2.27 as indicative of poor outcome [21]. Duran et al., reported that improved postoperative semen parameters were 2.9 times more likely when preoperative NLR was <2.02 [22]. This variability in cut-offs suggests there is not yet a universal definition of “elevated NLR” in the context of varicocelectomy. It highlights the need for standardization or larger studies to determine an appropriate threshold for clinical use. Nonetheless, despite different cut-off values, the association was uniform across studies, with lower NLR predicting better surgical outcomes, and reinforcing that NLR reflects an inflammatory state relevant to varicocele pathophysiology and recovery.
All included studies measured NLR only preoperatively, typically at the time of the initial infertility evaluation or just before surgery. None of the studies obtained serial or postoperative NLR measurements, so our analysis is based on a single pre-surgical NLR value as a predictor. We have clarified in our review that NLR was assessed once before varicocelectomy in each study (as part of routine blood work-up) and not repeated afterwards. The timing of outcome assessment (semen analysis) was relatively consistent. In most reports, a follow-up semen analysis was performed about 6 months after surgery to evaluate improvement, which aligns with the typical timeframe for spermatogenesis to respond to interventions. This indicates that NLR and semen analysis were well separated in time with NLR reflecting pre-surgical inflammatory status, and semen analysis reflecting the subsequent fertility outcome after an adequate recovery period.
Another important aspect we expanded upon is how semen analysis outcomes were defined and evaluated across studies. The included investigations varied slightly in their outcome definitions. Three studies defined surgical success in terms of increases in the total motile sperm count, which istypically a >50% increase in TMSC on postoperative analysis (with a >100% increase required for very low baseline counts) [19, 20, 22]. In contrast, one study (Omer et al.) took a more stringent approach and required normalization of all seminal parameters (concentration, motility, and morphology) at 6 months after a surgical operation to consider the varicocelectomy successful [21].
Among the included studies, compliance with standardized semen analysis protocols as per the World Health Organization (WHO) was variable. Omer et al. explicitly stated that semen analysis was conducted according to WHO guidelines, with patients advised to abstain from sexual intercourse for at least three days, and samples analyzed within one hour of liquefaction [21]. Their study also conducted two semen analyses before and after surgery and uniquely reported spontaneous pregnancy outcomes during follow-up. In contrast, Kandevani et al. reported semen collection after 2-3 days of abstinence. They evaluated key parameters, including total motile sperm count (TMSC) and morphology, but did not specify adherence to WHO protocols or repeat testing postoperatively [20]. Ates et al. conducted at least two semen analyses preoperatively but selected only the sample with the highest TMSC as the baseline; however, they did not mention abstinence periods or whether WHO guidelines were followed [19].
The patient populations in the included studies covered a spectrum of clinical varicocele severities. Most patients had grade II-III varicoceles, with a minority of grade I cases (or none, in one study that only included grade ≥II). We have noted in the revised text that none of the studies performed a stratified analysis to determine if NLR’s predictive value holds true across different varicocele grades. This is relevant because prior research suggests that higher-grade varicoceles may cause more severe impairment and potentially greater postoperative improvement in sperm parameters. For example, Wang et al., found that varicocele grade influenced the magnitude of semen improvement after repair [8]. Given this context, one might expect the usefulness of NLR as a prognostic marker could vary by grade (e.g., it might be particularly relevant in high-grade varicoceles where inflammation is more pronounced).
We also noted the absence of baseline patient data and other potential confounders in the included studies. Specifically, none of the studies reported on patients’ baseline hormonal profiles (such as follicle-stimulating hormone, luteinizing hormone, or testosterone levels) or other fertility-related markers. These hormonal factors are known to influence spermatogenesis and may potentially impact varicocelectomy results [11, 12, 29, 30]. Elevated NLR is a non-specific marker of inflammation that could stem from sources unrelated to varicocele. For example, an unseen genitourinary infection or systemic inflammatory condition could raise NLR and confound its relationship with varicocelectomy outcome. The included studies largely assumed that NLR reflected the inflammation associated with varicocele or the general health status of the patient, but without explicit examination of the causes of high NLR, this remains an assumption.
Another point now highlighted is that none of the included studies measured NLR again after surgery. It would be interesting to know if varicocelectomy, by alleviating the varicocele, leads to a reduction in systemic inflammation (and thus a drop in NLR over time) or if NLR remains unchanged. Unfortunately, the data on this finding is lacking.
With regard to other prognostic factors beyond NLR, obesity is also associated with increased incidence of low sperm concentration and low progressively motile sperm count. Hammoud et al. conducted a study related to infertility treatment [31]. Additionally, obesity contributes to cell damage. The compounds secreted by adipose tissue are essential for certain biological processes, making it a vital secretory organ for the body. Excessive adipose tissue storage is a hallmark of obesity, which leads to increased adipokine secretion. As a result, the body produces different effects and may develop resistance to these effects, as is the case with leptin. Along with adipokines, we also discovered an excess of reactive oxygen species (ROS), which harm cellular structures and, when combined with a lack of NO, cause fat to gradually accumulate and, ultimately, lead to the emergence of various diseases [13, 32].
Additionally, a retrospective review of patient clinical data was conducted by Miao et al. in 2024 [33]. Systemic immune-inflammation index (SII), neutrophil-lymphocyte ratio (NLR), platelet-lymphocyte ratio (PLR), and body mass index (BMI) were all statistically significantly different between the varicocele and non-varicocele group [33]. The study by Samplaski showed that men with bigger varicoceles showed the biggest improvements in semen characteristics [26]. Inflammatory disorders are well-recognized contributors to male infertility. Research by Nallella et al. (2004) demonstrated that levels of IL-6 and ROS were elevated in patients suffering from varicocele, while total antioxidant capacity was found to be reduced [15]. This indicates that the pro-inflammatory cytokine IL-6 and oxidative stress may play a role in the infertility mechanisms observed in these individuals. Additionally, it has been noted that IL-18, which is significantly elevated in men with varicocele, could activate neutrophils that contribute to the development of infertility and varicocele through inflammatory processes. Furthermore, IL-37, known for its anti-inflammatory properties, has been shown to bind with IL-18 binding protein, reducing the pro-inflammatory effects of IL-18 and thereby potentially enhancing sperm motility by alleviating inflammation related to IL-37 in cases of varicocele-related infertility [15].
In order to predict the likelihood of infertility in patients with varicocele, Wang et al., conducted research to create a nomogram employing hemogram inflammatory indicators [34]. Out of the total 162 patients, 81 were infertile and 81 were fertile. The systemic inflammation response index, neutrophil/lymphocyte ratio (NLR), platelet/lymphocyte ratio (PLR), MPV/platelet ratio (MPVPR), erythrocytes, monocytes, lymphocytes, red cell distribution width (RDW), mean erythrocyte volume (MCV), mean platelet volume (MPV), and platelet distribution width (PDW) all showed statistically significant differences between the two groups. SIRI, NLR, PDW, and erythrocyte were found to be independent risk factors for infertility. In light of the findings, we advise VC patients to be screened for infertility using these inflammatory parameters as indicators. Yagmur conducted a study on the function of inflammatory markers in patients with varicocele and found similar results [35].
NLR, an indicator of inflammation, has been investigated across various types of cancer. It has been identified as a prognostic marker in urothelial carcinoma, hepatocellular carcinoma, and several cancers, including gastric, breast, and pancreatic cancer [36]. Research consistently demonstrated that elevated levels of NLR are associated with worse outcomes in these malignancies [37]. Additionally, NLR has been recognized as a predictor of morbidity and mortality in vascular diseases [38, 39]. In 2017, Mosmiller et al., proposed the potential utility of NLR in assessing chronic venous insufficiency, marking the first instance of its consideration in this context [40]. Furthermore, a study suggests that NLR may serve as an indicator of Chronic Venous Insufficiency (CVI) severity .
The cumulative evidence from these studies underscores the importance of incorporating NLR and other hematologic markers into the pre-operative assessment of infertile men with varicocele. By utilizing these markers as predictive tools, clinicians can more effectively identify patients who will benefit the most from varicocele surgery, thereby optimizing treatment outcomes and enhancing overall fertility prospects [19-22].
This review is limited by the small number of included studies (n=4) and sample size (442 patients), with three being retrospective in design. Considerable heterogeneity exists across studies in NLR cut-off values, in definitions of surgical success, and patient characteristics, limiting comparability and generalizability. Most studies lacked long-term follow-up and did not report pregnancy or live birth outcomes, relying solely on short-term semen parameters as surrogate endpoints. Furthermore, only one study followed WHO semen analysis protocols, and hormonal or inflammatory confounders were often unreported. These limitations suggest the findings should be interpreted as hypothesis-generating, underscoring the need for larger, standardized, prospective studies with clinically meaningful endpoints.
CONCLUSION
In conclusion, the findings from the discussed studies highlight the potential of the NLR as a predictive marker for the success of varicocelectomy in improving male fertility outcomes. Elevated NLR levels were associated with varicocele surgery failure, suggesting the detrimental impact of inflammation on treatment efficacy. Pre-operative assessment of NLR levels may aid in identifying candidates likely to benefit from varicocelectomy, optimizing treatment outcomes.
AUTHORS’ CONTRIBUTIONS
It is hereby acknowledged that all authors have accepted responsibility for the manuscript's content and consented to its submission. They have meticulously reviewed all results and unanimously approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| NLR | = Neutrophil-to-Lymphocyte Ratio |
| ROS | = Reactive Oxygen Species |
| ISV | = Internal Spermatic Vein |
| PRISMA | = Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| MeSH | = Medical Subject Headings |
| BMI | = Body Mass Index |
| TMSC | = Total Motile Sperm Count |
| MPV | = Mean Platelet Volume |
| MLR | = Monocyte-to-Lymphocyte Ratio |
| PLR | = Platelet-to-Lymphocyte Ratio |
| SII | = Systemic Immune-Inflammation Index |
| SIRI | = Systemic Inflammation Response Index |
| MPVPR | = Mean Platelet Volume-to-Platelet Ratio |
| RDW | = Red Cell Distribution Width |
| MCV | = Mean Corpuscular Volume |
| PDW | = Platelet Distribution Width |
| WHO | = World Health Organization |
| IL | = Interleukin |
| NO | = Nitric Oxide |
| PPV | = Positive Predictive Value |
| NPV | = Negative Predictive Value |
| AUC | = Area Under the Curve |
| CI | = Confidence Interval |
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.
ACKNOWLEDGEMENTS
Declared none.

