All published articles of this journal are available on ScienceDirect.

Prospective Cohort Study on the Long-term Impact of Intraoperative Heparin in Radiocephalic Arteriovenous Fistulas
Authors Info & Affiliations
Abstract
Introduction
Short-term randomized trials suggest that intraoperative systemic heparin improves arteriovenous fistula (AVF) patency, but long-term outcomes remain unclear. This study reports the five-year follow-up of a previously published double-blinded randomized trial on systemic heparin during AVF creation.
Methods
Eighty-eight patients from the original trial (July 2015–July 2016) were included, equally randomized into the heparin and control groups. Long-term outcomes (July 2016–July 2022) were obtained from electronic hospital records, dialysis centers, and telephone follow-up. Primary endpoints were AVF patency, secondary interventions, mortality, and renal transplantation.
Results
Seventy-two patients were available for final analysis. The median age was 57.5 years. Primary patency was superior in the heparin group during the first two years, with borderline significance at year 1 (p-value = 0.06) and statistical significance at year 2 (p-value = 0.019). Beyond year 2, no significant differences were observed. Mortality was higher in the control group (12 vs. 9 deaths), with cardiac events accounting for 32% of all deaths. Secondary interventions were more frequent in the control group, although the difference was not statistically significant.
Discussion
Intraoperative systemic heparin demonstrated a clear benefit in early AVF patency, which may improve uninterrupted dialysis access in patients with end-stage renal failure. However, the effect diminished after two years, and long-term outcomes were influenced by mortality and loss to follow-up.
Conclusion
Systemic heparin improves primary AVF patency during the first two years, supporting its role in early access preservation. Larger multicenter studies are warranted to validate these findings.
1. INTRODUCTION
End-stage renal failure (ESRF) is a growing global healthcare challenge. To ensure uninterrupted hemodialysis and improve patient outcomes, arteriovenous fistulas (AVFs) remain the preferred long-term access, as recommended by the 2019 Kidney Disease Outcomes Quality Initiative (KDOQI) guidelines [1]. Due to a shortage of kidney donors and the increasing number of patients requiring renal replacement therapy, maintaining a durable and functional vascular access is critical.
Several strategies have been explored to prolong AVF functionality, including refined surgical techniques, cannulation protocols, intraoperative medications, and surveillance practices [2]. Systemic heparin is one such intervention that has been widely studied for its anticoagulant effect during vascular procedures. A number of randomized controlled trials (RCTs) have reported conflicting results on the role of intraoperative heparin in improving early AVF patency and reducing thrombosis [3].
In 2015, we conducted a double-blinded randomized trial evaluating the effects of systemic heparin (5000U) during radiocephalic AVF creation [4]. Results showed reduced early thrombosis and higher maturation rates in the heparin group, without an associated increase in bleeding complications.
However, almost all prior studies, including our own, were limited to short-term outcomes, with follow-up ranging from 24 hours to 3 months [4-9]. Long-term data on primary and secondary AVF patency and patient survival are sparse. This study addresses that gap by evaluating the 5-year outcomes of the original trial cohort, with a focus on fistula durability, reintervention rates, mortality, and transplant status.
2. METHODOLOGY
2.1. Study Design and Population
This study represents a 5-year prospective follow-up (2017–2022) of a previously published double-blinded randomized controlled trial conducted at a tertiary hospital in Malaysia. The original trial enrolled 90 patients with end-stage renal failure (ESRF) between July 2015 and July 2016 who underwent radiocephalic arteriovenous fistula (AVF) creation. A total of 88 patients completed the initial study and were eligible for inclusion in this long-term follow-up.
Inclusion criteria for the original trial were:
- Age ≥18 years
- Diagnosis of ESRF requiring AVF creation
- Artery and vein diameter >2 mm on preoperative duplex ultrasound
Exclusion criteria included the following:
- History of bleeding disorders
- Use of therapeutic anticoagulation
- AVF creation at any site other than the radiocephalic location
Randomization was performed using sealed envelope block randomization in a 1:1 ratio. Patients were assigned to receive either 5000 units of systemic intravenous heparin or normal saline (placebo) during AVF creation. Surgical procedures were carried out by either senior surgeons (≥100 AVFs performed) or junior surgeons (<100 AVFs performed).
Follow-up data were obtained through the following:
- Electronic hospital and dialysis center records
- Telephone interviews with patients or caregivers
- Outpatient clinic documentation
Patients were followed until one of the following endpoints: AVF failure, kidney transplantation, death, or completion of the 5-year follow-up period. Patients lost to follow-up or with incomplete medical records were also excluded from the final analysis.
The following data were collected:
- Demographics and comorbidities
- AVF outcomes, including primary and secondary patency
- Secondary interventions, including fistuloplasty, central venoplasty, and proximalization
- Cause of death, when applicable
2.1.1. Definitions
- Primary patency: This entails the time from AVF creation to first access failure or the need for an intervention to maintain function
- Secondary patency: This entails the time from AVF creation to permanent access abandonment, including successful restoration following any intervention
2.2. Statistical Analysis
Statistical analysis was performed using GraphPad Prism (version 8.2.1) and SPSS (version 28.0). The normality of data was assessed using the Shapiro-Wilk test. Non-parametric tests were applied as appropriate. Categorical variables were analyzed using Fisher’s exact test or the Chi-square test.
Kaplan–Meier survival curves were generated to estimate AVF patency over time, and groups were compared using the log-rank (Mantel-Cox) test. Multivariate Cox proportional hazards regression was conducted to evaluate independent predictors of patency, despite non-significant univariate results, to control for potential confounders and explore latent interaction effects. Ap-value <0.05 was considered statistically significant.
The original sample size (n=90) was calculated to detect a 30% reduction in early thrombosis with 80% power and a 5% alpha error. While appropriate for early outcomes, the statistical power for long-term comparisons was likely reduced due to patient attrition and mortality during the follow-up period.
3. RESULTS
Of the 88 patients who completed the original randomized controlled trial, 72 were successfully followed for a minimum of five years. Ten patients were lost to follow-up, and six were excluded due to incomplete data during the follow-up period, four from the control group and two from the intervention group. As a result, the final analysis included 39 patients in the control group and 33 in the intervention (heparin) group. The median age of the cohort was 57.5 years (range, 27-79), with 42% female and 58% male. Both groups had a high prevalence of diabetes mellitus and hypertension, with no statistically significant differences in baseline characteristics, which are summarized in Table 1.
Regarding patency outcomes, the intervention group exhibited better overall primary and secondary patency rates compared to the control group over the five-year period. However, the overall difference was not statistically significant (p-value = 0.08). When examined on a year-by-year basis, primary patency in the intervention group was notably superior during the first two years. In year 1, the difference approached statistical significance (p-value = 0.06), and in year 2, the result was statistically significant (p-value = 0.019). Beyond the second year, however, the Kaplan–Meier survival curves for the two groups converged, and the difference in primary patency lost statistical significance. These survival trends are depicted in Fig. (1), which also includes the number of patients at risk over time.
Several secondary interventions were required during the follow-up period. Fistuloplasty was performed in five patients in the control group and two in the intervention group (p-value = 0.70). Central venoplasty was performed in three patients from the control group and two from the intervention group. One proximalization procedure was recorded, and it occurred in the intervention group. Although secondary interventions were more common in the control group, the differences were not statistically significant, as detailed in Table 1.
Over the five-year follow-up, a total of 21 patients died, 12 from the control group and 9 from the intervention group. Cardiac events were the most frequent cause of death, accounting for 32% of cases. Pneumonia and malignancy were the second most common causes, each representing approximately 20% of total deaths. These findings are illustrated in Fig. (2).
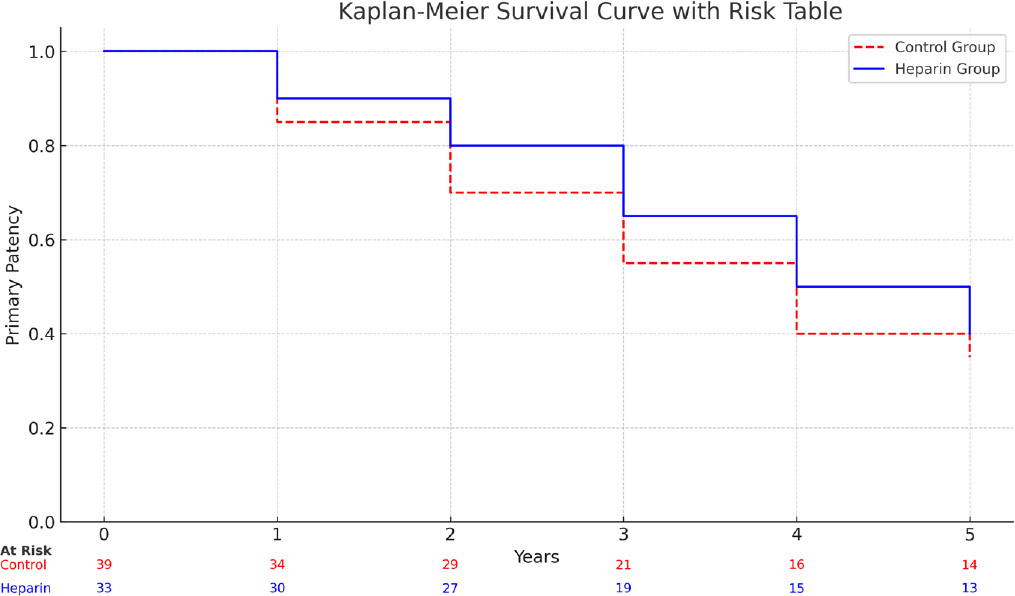
Survival curve of the primary patency between the control and the heparin group. The survival curves differed for the first two years (p-value = 0.019) but were similar afterwards (p-value = 0.08).
| Patient Characteristics | Control (N = 39) | Intervention (N = 33) | p-value* |
|---|---|---|---|
| Age (Median with range) | 57 (27 to 77) | 58 (29 to 79) | 0.51 |
| Dialysis (N, %) | 29 (88) | 24 (90) | 0.78 |
| Gender (F, %) | 12 (37) | 21 (46.6) | 0.53 |
| Diabetes (N) | 29 (88) | 41 (91.1) | 0.78 |
| Hypertension | 29 (88) | 45 (100.0) | 0.55 |
| History of Thrombus | 8 (26) | 2 (8) | 0.08 |
| Ischemic heart disease | 1 (4) | 1 (2) | 0.84 |
| Peripheral vascular disease | 10 (31) | 7 (26) | 0.89 |
| On Aspirin | 2 (8) | 4 (15) | 0.62 |
| Secondary procedures | - | - | - |
| Fistuloplasty | 5 (14) | 2 (8) | 0.70 |
| Central venoplasty | 3 (9) | 2 (7) | 0.60 |
| Proximalisation | 0 (0.0) | 1 (4) | 0.60 |
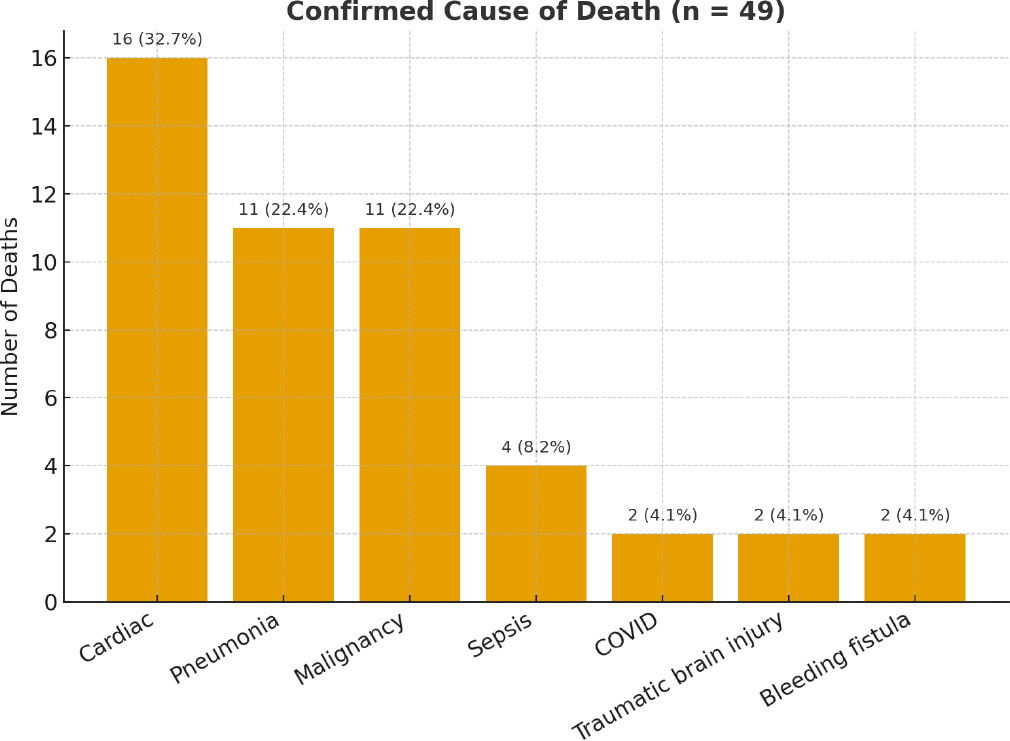
Causes of death of the study participants.
| Study Parameters | p-value | 95% CI |
|---|---|---|
| History of previous fistula | 0.548 | 0.359 to 2.450 |
| Dialysis | 0.263 | 0.613 to 3.468 |
| Diabetes | 0.557 | 0.279 to 2.157 |
| Antiplatlet | 0.647 | 0.263 to 23.009 |
| Age | 0.292 | 0.993 to 1.125 |
| Study Parameters | B-coefficient | Standard Error | p-value |
|---|---|---|---|
| History of previous fistula | .032 | .135 | .811 |
| Dialysis | .136 | .118 | .255 |
| Diabetes | .020 | .183 | .914 |
| Hypertension | .179 | .239 | .457 |
| Ischaemic heart disease | .439 | .298 | .144 |
| Peripheral vascular disease | .041 | .121 | .737 |
| Sex | .126 | .110 | .310 |
Univariate regression analysis was conducted to explore potential predictors of primary patency, including age, diabetes status, dialysis dependence, prior AVF creation, and use of antiplatelets. None of these variables were found to be statistically significant predictors of outcome, as presented in Table 2. Despite the lack of significance in the univariate analysis, multivariate Cox regression was conducted to control for potential confounding and to identify any hidden interactions between variables. This analysis similarly revealed no independent predictors of primary patency (Table 3). The rationale for conducting multivariate modelling was to provide adjusted estimates while accounting for potential collinearity and suppressor effects that might not be evident in univariate testing.
4. DISCUSSION
Arteriovenous fistula (AVF) remains the vascular access of choice for long-term hemodialysis, in line with international guidelines, such as KDOQI 2019 [10]. Despite its advantages, primary AVF failure rates remain high, ranging from 20% to 40%, with early thrombosis being a major contributor [11]. This study aimed to evaluate whether systemic intraoperative heparin improves long-term patency of radiocephalic AVFs.
Our findings demonstrate that systemic heparin significantly improves primary patency within the first two years after creation, although the benefit diminishes thereafter. This suggests that intraoperative heparin may confer early thrombo-protection during the critical period of AVF maturation, which is supported by our previous short-term trial results [11].
Short-term benefits of systemic heparin during AVF surgery have been shown in several RCTs, albeit with heterogeneous results and varying definitions of patency [12]. Our findings align with the recent systematic review, which highlighted potential early patency benefits but emphasized the lack of standardized protocols and limited long-term data [12]. Similarly, the European Renal Best Practice guidelines (2019) caution against routine heparin use due to the associated bleeding risks and insufficient high-quality evidence [13].
In our study, systemic heparin was not associated with an increased incidence of bleeding complications, and no hematomas requiring intervention were reported during the initial trial. However, this safety profile must be interpreted cautiously, especially in settings with higher hemorrhagic risk, such as advanced age, concurrent antiplatelet use, or poor vascular integrity.
The finding that systemic heparin significantly improved patency only in the first two years is particularly relevant. The USRDS data indicate that median survival for dialysis patients is often under five years [14], making early AVF function critically important for quality of life and reducing the need for central venous catheters.
Although more patients in the heparin group were on antiplatelets during follow-up, the difference was not statistically significant. Evidence on the use of antiplatelets post-AVF creation remains mixed. A recent Cochrane review concluded that the overall quality of evidence is low due to short follow-up and inter-study heterogeneity. Similarly, Su et al. showed that antiplatelets reduce cardiovascular events by about 15%, but their effect on AVF patency is unclear, especially in dialysis-dependent ESRF patients [15].
The radiocephalic site was specifically chosen for this study due to its high early failure rate and distal location, which preserves more proximal veins for future use. Previous studies, such as those by Nguyen et al., reported maturation rates as low as 50% in radiocephalic AVFs compared to 68% in brachiocephalic AVFs [16]. The smaller vessel caliber at the wrist likely contributes to early thrombosis, making interventions, such as systemic heparin, more impactful at this site.
The mortality rate during this study was significant, with cardiac events as the leading cause, consistent with previous ESRF cohort studies [17]. Although the proportion of patients with documented ischemic heart disease was low at baseline, it is likely underdiagnosed in this high-risk population. The high mortality underscores the importance of early and effective AVF function in maximizing dialysis efficiency during a limited patient lifespan.
Loss to follow-up and inconsistent post-operative care (across dialysis centers) are major limitations. After AVF creation, patients were followed by nephrologists at different centers, introducing variability in cannulation technique, access surveillance, and complication management. This heterogeneity may have influenced long-term outcomes.
5. STUDY LIMITATIONS
This study has several limitations that should be considered when interpreting the findings. First, approximately 20% of the original cohort was either lost to follow-up or excluded due to incomplete records or renal transplantation. This level of attrition reduces the statistical power for long-term comparisons and may introduce selection bias, particularly in survival and patency analyses.
Second, the mortality rate during the five-year follow-up was considerable, with 21 patients dying over the study period. This significantly reduced the number of participants contributing data to later time points, limiting the strength of conclusions about long-term outcomes. Although this mirrors real-world survival rates in the dialysis population, it nonetheless restricts the robustness of extended follow-up data.
Third, the study was subject to variability in postoperative care. Patients received dialysis across multiple centers with differing protocols for vascular access surveillance, cannulation techniques, and access maintenance. This heterogeneity may have affected AVF outcomes and introduced confounding variables that were not standardized or controlled for in the analysis.
Another limitation involves the non-standardized use of antiplatelet agents following AVF creation. While a greater number of patients in the intervention group were on antiplatelets, the difference was not statistically significant. However, the presence or absence of antiplatelet therapy could have influenced patency independently of intraoperative heparin use, confounding the effect size attributed to the intervention.
Additionally, the original sample size was calculated to detect early thrombosis differences, rather than being powered for long-term patency or mortality outcomes. The reduced number of patients remaining after two years limits the statistical validity of longer-term comparisons and subgroup analyses.
Finally, the generalizability of the study findings is limited. This was a single-centre study focused solely on radiocephalic AVFs, and as such, the results may not be applicable to other AVF configurations, such as brachiocephalic or basilic vein transpositions, or to broader ESRF populations with differing demographic or clinical characteristics.
CONCLUSION
This 5-year follow-up study supports the early benefit of intraoperative systemic heparin in improving primary patency of radiocephalic arteriovenous fistulas in ESRF patients. Specifically, systemic heparin demonstrated statistically significant superiority in the first two years post-creation, a critical window for AVF maturation and durability.
However, this benefit was not sustained beyond year two, and the long-term advantages were attenuated by substantial patient attrition, mortality, and non-standardized dialysis care. Furthermore, while systemic heparin was not associated with increased bleeding complications in this study, its use should be carefully considered on a case-by-case basis, especially in patients with elevated hemorrhagic risk.
In light of these findings, systemic heparin may serve as a useful adjunct in select patients undergoing radiocephalic AVF creation. However, current evidence, including systematic reviews and international guidelines, does not support its routine use. Future multi-centre randomized trials with larger sample sizes, standardized post-operative care, and extended follow-up are essential to validate these results and better define the role of systemic heparin in vascular access surgery.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contributions to the paper as follows: K.A.: Study conception and design; P.M.P.: Data analysis or interpretation; C.L.G. and H.T.: Draft manuscript. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| AVF | = Arteriovenous Fistula |
| USRDS | = United States Renal Data System |
| KDOQI | = The National Kidney Foundation's Kidney Disease Outcomes Quality Initiative |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the National Malaysian Research Registry, Malaysia (RSCH ID-23-02752-UUR).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Written informed consent was obtained from all participants at the time of enrolment.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available at [1. Aimanan K. Heparin study. Zenodo; 2025.], reference number [https://doi.org/10.5281/zenodo.17201565].
ACKNOWLEDGEMENTS
The authors would like to express their sincere gratitude to the Director General of Health Malaysia for his permission to publish this research. They also thank the surgical, nephrology, and dialysis teams involved in the care of these patients. Special thanks to the patients and their families for their participation and cooperation during the extended follow-up period.

