All published articles of this journal are available on ScienceDirect.

Pitfall of Renal Vascular Embolization in Managing Recurrent Hematuria Post-Nephrolithotomy: A Case Report
Authors Info & Affiliations
Abstract
Introduction
Renal vascular embolization (RVE) is an advanced, minimally invasive procedure frequently employed in the clinical management of recurrent haematuria, particularly in patients with underlying vascular abnormalities contributing to this condition. Although renal vascular embolization (RVE) has demonstrated considerable efficacy in mitigating the symptoms associated with haematuria, it can pose substantial challenges.
Case Presentation
The case report shows a patient with a history of nephrolithiasis who underwent open nephrolithotomy for a right renal calculus. After the procedure, the patient developed haematuria and underwent renal vascular embolization. Three weeks post-procedure, the patient returned with severe haematuria and the second renal vascular embolization procedure was performed. The condition indicates undetected vascular abnormalities during the procedure, which resulted in an incomplete embolization. This comprehensive analysis of the case report underscores the critical importance of conducting thorough pre-procedural imaging, ensuring precise catheter placement throughout the intervention, and the urgent need to identify all pertinent vascular structures that may relate to the patient's condition. Furthermore, this case illustrates the potential implications of overlooking anatomical variations in the renal vasculature, which can adversely affect treatment efficacy and patient recovery.
Conclusion
Pre-embolization CT angiography is essential in managing recurrent hematuria following nephrolithotomy to identify all potential sources of hemorrhage and all feeding vessels, including accessory arteries. Selective angiography may further enhance the accuracy of vascular mapping.
1. INTRODUCTION
Renal vascular embolization (RVE) is a novel and minimally invasive procedure specifically crafted for the adept administration and resolution of acute renal bleeding, thereby serving as a valuable option against standard surgical interventions that could pose higher risks and longer recovery phases. Over the years, increased clinical experience and advancements in imaging methods, catheter technology, and various embolic materials have made RVE much more effective for a broader range of issues, such as kidney diseases and injuries that may occur during planned surgeries or urgent medical situations. Acute renal bleeding frequently presents as a critical emergency in the field of urology. It is a serious condition that can arise from multiple underlying factors, including both closed and open renal trauma, and it can severely compromise renal function and patient stability. Renal vascular injuries can happen during several medical procedures, including renal biopsies, percutaneous nephrolithotomy (PCNL), or percutaneous nephrostomy (PCN) [1, 2]. Also, renal tumors like renal angiomyolipoma and renal cell carcinoma, when combined with renal arteriovenous malformations, make acute renal bleeding much more common. This shows how important it is to find and treat these problems quickly to lower the risk of complications. These causes of bleeding can manifest in various ways, such as aneurysms, pseudoaneurysms (PAs), blood outflow, arteriovenous fistulas (AVFs), and perinephric hematomas [3-5].
Clinical signs of bleeding can manifest in various ways, such as apparent hematuria or the occurrence of perirenal hematomas. In most situations, these occurrences of hemorrhaging are self-resolving, permitting the application of non-invasive management techniques successfully without requiring surgical measures. However, when there is continuous hematuria and massive or persistent bleeding, conservative treatment methods may not be effective, increasing the risk of recurrence and requiring more aggressive therapeutic measures. Consequently, these conditions usually need non-conservative treatments to stop the bleeding. These can include open surgery or the selective use of renal vascular embolization (RVE) methods to achieve hemostatic success [6, 7]. Despite the widespread recognition of renal vascular embolization's effectiveness in managing renal bleeding, it is important to acknowledge the challenges and complications that may occur during the procedure. The overall success of the embolization protocol depends on being able to get clear and accurate imaging before the procedure. This is due to the need to identify all potential sources of bleeding prior to the intervention. This case report showcases a patient managing recurrent hematuria with RVE, emphasizing the procedural pitfalls resulting from the failure to perform a comprehensive CT angiography prior to the embolization procedure. This oversight led to an incomplete embolization, which ultimately resulted in the recurrence of symptoms and necessitated further medical interventions to address the ongoing bleeding complications. This report aims to understand these pitfalls and underscore the necessity for careful planning and follow-up to prevent incomplete embolization and enhance patient safety.
2. CASE REPORT
2.1. Patient Information
A 49-year-old male with a history of nephrolithiasis underwent open nephrolithotomy for right renal calculus. The initial procedure was without complications, but the patient developed significant hematuria 1 week after the procedure. There were no complaints of fever, nausea, vomiting, or shortness of breath. The patient also complained of right flank pain.
2.2. Clinical Findings
The physical examination during hospitalization revealed no abnormalities in the patient's pulmonary, cardiac, or limb systems or vital signs. In the laboratory, the erythrocyte count was 3.55 × 10^6/uL, the white blood cell count was 6.55 × 10^3/uL, the hemoglobin level was 9.9 g/dL, the urea level was 17.0 mg/dL, and the serum creatinine level was 1.4 mg/dL. The results from all subsequent tests, including bleeding time, blood coagulation time, and plasma electrolytes, were within normal limits.
2.3. Diagnostic Assessment
The Doppler ultrasound showed decreased vascularization in the right kidney with mild hydronephrosis (Fig. 1). Based on the symptoms, the team suspected a renal arteriovenous fistula and proceeded with renal embolization without prior CT angiography.
2.4. Therapeutic Intervention
In the first procedure, we found a single pseudoaneurysm originating from the right renal middle pole segmental artery during the embolization procedure. We used VortX pushable coils (3.3 mm and 4.0 mm) and PVA 600 to do superselective embolization on the right renal middle pole segmental artery branch (Fig. 2). While the main artery, the right renal artery, remained patent, the right renal segmental artery underwent significant embolization. The immediate outcome was favorable, with a cessation of visible bleeding. The patient also received antibiotic therapy, analgesics, and injection hemostasis; underwent blood clot evacuation and received red cell transfusions.
2.5. Follow-up and Outcomes
Three weeks post-procedure, the patient returned with severe hematuria and anemia. The physical evaluation during hospitalization revealed no abnormalities in the lung, cardiac, or limb examinations and the vital signs. The laboratory result of the erythrocyte was 2.75 × 10^6/uL, with the leukocyte value recorded at 7.4 × 10^3/uL and hemoglobin measured at 7.5 g/dL, urea levels at 12.0 mg/dL, and serum creatinine concentration at 1.6 mg/dL. The outcomes of all subsequent tests exhibited normal findings, including bleeding time, blood coagulation time, and plasma electrolytes. We assessed the patient for recurrent hematuria and a suspected pseudoaneurysm in the right renal artery. The patient underwent an ultrasound examination, which showed two-way flow with a “yin-yang sign” that could be a pseudoaneurysm in the right kidney and moderate hydronephrosis in the right kidney with a DJ stent in situ (Fig. 3). Due to recurrent hematuria, we conducted a second angiography and embolization again without prior CT angiography.
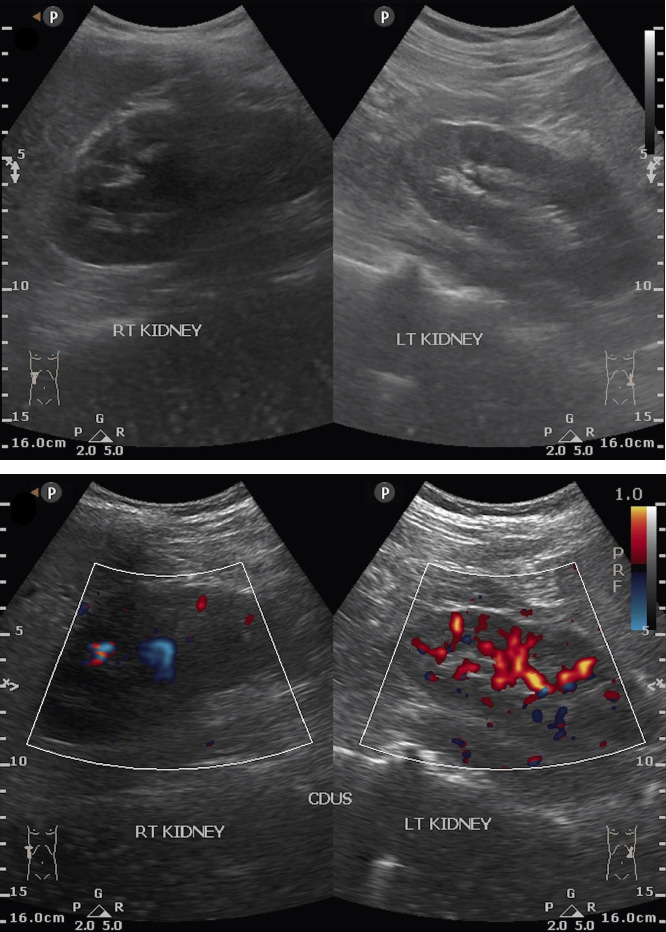
Pre-embolization ultrasound showing a decrease in vascularization in the right kidney with moderate hydronephrosis.
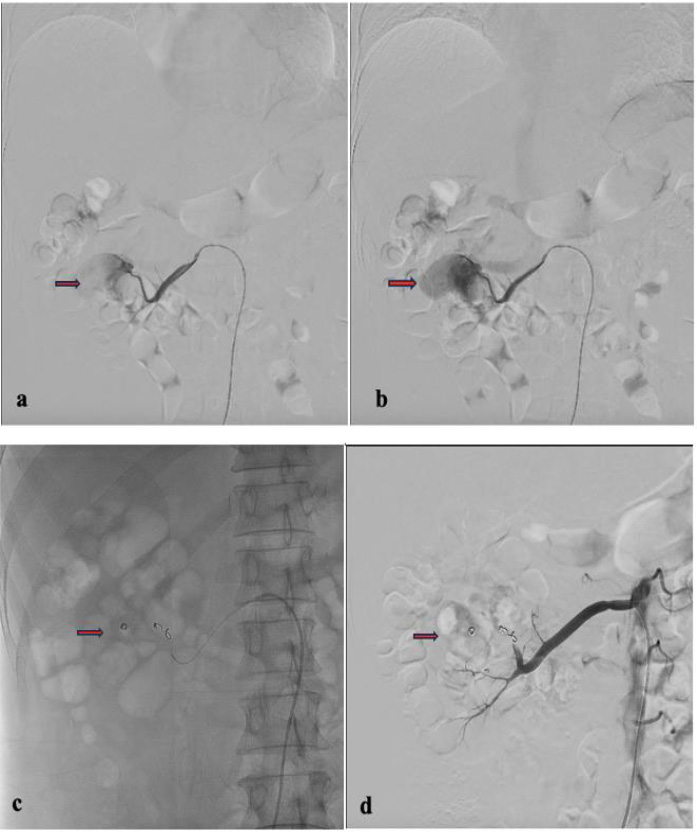
Angiography with a Cobra catheter and microcatheter. (a, b) Pseudoaneurysm in the right renal middle pole segmental artery; (c) Superselective embolization; (d) Angiography after embolization showed the bleeding artery is successfully occluded.

Ultrasound image post embolization with recurrent hematuria.
In this second procedure, we also performed the puncture on the right femoral using the Seldinger technique, which followed the same procedure as the first embolization. We proceeded with the installation of a 5F introducer sheath, which included a guide wire. We navigated the 5F Cobra catheter and guide wire to the right external iliac artery, the right common iliac artery, the bifurcation, and the abdominal aorta. We positioned a 2.7F progreat microcatheter and guided it to the right renal artery.
A contrast test was performed that revealed the presence of another pseudoaneurysm. The right renal segmental artery, located in the upper pole of the right kidney, appeared to be the source of the pseudoaneurysm, which the first embolization failed to find or treat. We used 4 mm and 5 mm Coiling Vortx 18 pushable and a PVA 500-710 to target the right renal segmental artery branch and the upper pole of the right kidney. We performed a contrast test and observed significant embolization of the right renal segmental artery, which ultimately resolved the hematuria (Fig. 4). After receiving treatment, the patient's complaints decreased, and hematuria no longer occurred.
3. DISCUSSION
The prevalence of severe renal hemorrhagic complications following surgical procedures can escalate to a concerning 9.5%, highlighting a significant risk factor for patients undergoing such interventions. When bleeding lasts for a long time, it can lead to several other problems, such as cardiovascular collapse, acute renal impairment, and widespread clotting dysfunction, all of which can make it much harder for the patient to recover [8]. The surgical approach to fixing renal artery injuries is especially challenging in cases of hemodynamic instability, as such patients bear a greater risk of procedural failure and might end up needing a nephrectomy. Renal angiography is now a vital diagnostic method because of its accuracy in identifying vascular issues in the kidneys, particularly when considering renal vascular embolization (RVE) as a surgical alternative [9, 10]. Various cases of surgical complications to renal arteries, which could benefit from renal vascular embolization, include direct bleeding into the perirenal or subcapsular zones, potentially resulting in hematoma formation, and bleeding into the pelvicalyceal system, characterized by arteriocalyceal fistulas in addition to arteriovenous fistulas (AVFs) or pseudoaneurysms. Such complications may arise as a direct consequence of surgical manipulation involving renal vessels during procedures aimed at stone removal [11, 12].
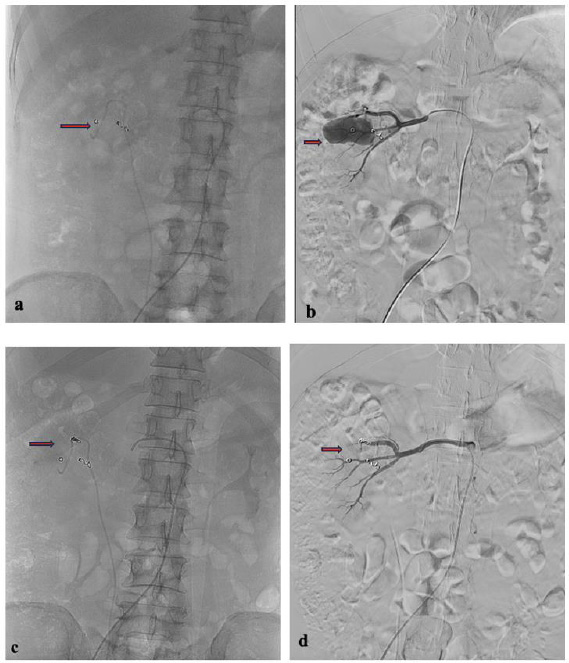
Second angiography with a cobra catheter and microcatheter. (a) Coil post first embolization procedure; (b) Pseudoaneurysm of the right renal upper pole segmental artery; (c) Super selective embolization; (d) A contrast test was performed, and the right renal segmental artery was seen to be significantly embolized.
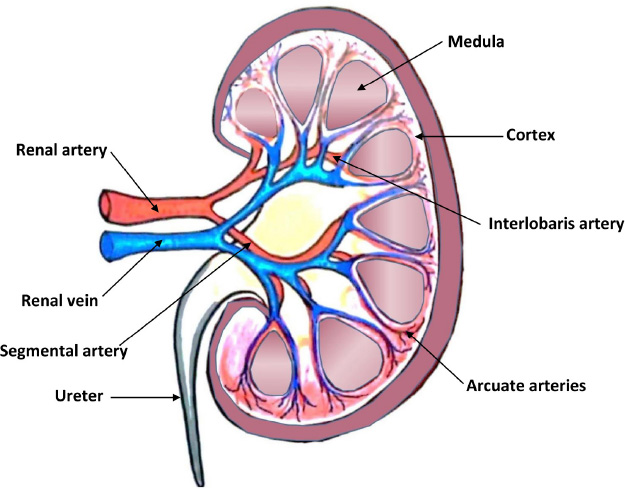
Anatomy of renal artery.
Most RVE procedures are performed via the femoral artery using arterial sheaths of 4–6F. Standard cobra or shepherd hook-shaped catheters can easily and effectively catheterize the renal arteries, as these tools are typically sufficient for selective embolization. Microcatheters enable superselective embolization, significantly reducing procedure morbidity and the volume of induced renal infarction [5, 13]. Typically, we employ coils to embolize large proximal bleeders and prefer polyvinyl alcohol (PVA) particles for smaller distal bleeding sources. We use glue as an alternative approach in cases involving hemodynamically unstable patients exhibiting an abnormal bleeding profile [2, 14, 15]. Once the embolization procedure is complete, we perform selective angiography to evaluate the effectiveness of arterial occlusion. At the same time, the catheter remains in the main renal artery, utilizing a manual injection of contrast media for optimal visualization [1].
Understanding the anatomy of the renal vasculature is crucial for pre-procedural planning of renal artery embolization [9]. The renal arteries originate from the aorta abdominalis, which is situated underneath the commencement of the superior mesenteric artery, typically between the superior endplate of L1 and the inferior endplate of L2 [15]. Adjacent to the renal hilum, each renal artery bifurcates into an anterior and a posterior branch and then bifurcates into the segmental arteries that supply the upper, middle, and lower poles (Fig. 5). Upon division into two, these segmental arteries transform into lobar, interlobar, arcuate, and interlobular arteries [9].
Approximately 75% of the population demonstrates the presence of a single renal artery on both sides. The remaining 25% exhibit renal artery duplication, with a higher prevalence on the right side. The angiographic evaluation of the principal renal artery may fail to delineate the region of clinical interest if the presence of an accessory renal artery that supplies the kidney is not recognized [16]. If imaging tests before the procedure fail to identify the common variation in anatomy known as the accessory renal arteries properly, it could lead to incomplete embolization and persistent hemorrhage despite attempts at embolization. We suggest using advanced imaging technologies like multi-phase computed tomography or magnetic resonance angiography to locate these vessels before embolization, thereby promoting a more comprehensive and targeted treatment plan [17].
Pre-embolization CT angiography is essential for the accurate location and characterization of vascular lesions responsible for recurrent hematuria after nephrolithotomy [18]. In emergency instances where CT angiography cannot be conducted promptly due to patient instability or logistical limitations, it may be necessary to move immediately to angiography and embolization. This method reduces delays and the hazards linked to patient transportation, which can worsen hemodynamic instability [19, 20]. In addition to angiography, renal ultrasonography is a valuable adjunct in the pre-embolization imaging workup. Renal ultrasonography offers multiple advantages as part of the pre-embolization assessment in patients with suspected renal vascular injury, particularly following nephrolithotomy. It enables early detection of vascular complications such as pseudoaneurysms, arteriovenous fistulas, and perirenal hematomas, which are important to identify prior to intervention. Unlike CT angiography, ultrasonography does not expose patients to ionizing radiation or nephrotoxic contrast agents, making it especially advantageous for individuals with renal insufficiency or a solitary kidney. The modality provides real-time, bedside evaluation, allowing for rapid assessment in unstable or critically ill patients. Additionally, ultrasonography can guide percutaneous embolization procedures directly, offering a safe alternative in high-risk cases where contrast use is contraindicated. Doppler ultrasound further contributes by assessing renal perfusion and blood flow dynamics, which aids in planning embolization strategies that preserve renal function. Finally, ultrasonography serves as a noninvasive tool for monitoring and follow-up after embolization, facilitating early detection of recurrent vascular lesions or new complications [21, 22]. Integrating ultrasonography into the pre-procedural workup enhances diagnostic accuracy and supports individualized patient management. This case exemplifies the potential pitfalls of conducting renal embolization without comprehensive pre-procedural imaging, especially computed tomography angiography [15]. CT angiography creates detailed maps of the blood vessels, which let doctors look closely at possible bleeding sources. In this case, reliance on Doppler ultrasound alone likely led to the missed pseudoaneurysm and subsequent treatment failure [23].
A thorough angiographic assessment before embolization is crucial for precisely identifying all feeding arteries and pseudoaneurysms, hence ensuring complete management of the hemorrhagic source. After embolization, it is important to do a follow-up angiography to check if the targeted areas are closed and to find any remaining or new pseudoaneurysms that could cause bleeding again. This two-step angiographic protocol reduces the risk of incomplete embolization and improves clinical outcomes by enabling prompt reintervention if necessary [1, 6].
CONCLUSION
Pre-embolization CT angiography is essential in managing recurrent hematuria following nephrolithotomy to identify all potential sources of hemorrhage and all feeding vessels, including accessory arteries. In instances of complexity, selective angiography may further enhance the accuracy of vascular mapping. In embolization techniques, using microcatheters for superselective embolization and embolic agents may improve accuracy and lower the risk of embolization going to the wrong place. To ensure the complete blockage of all feeding vessels, monitoring is necessary after the procedure.
AUTHORS’ CONTRIBUTIONS
The authors confirm contribution to the case report as follows: H.A., H.S.: Study conception and design; H.A., H.S., A.T. and A.S.: Management and data collection; H.A.: Draft manuscript preparation; H.S., A.T. and A.S.: Critical revision of the manuscript. All authors reviewed the manuscript and approved the final version.
LIST OF ABBREVIATIONS
| RVE | = Renal Vascular Embolization |
| CT | = Computed Tomography |
| PCNL | = Percutaneous Nephrolithotomy |
| PCN | = Percutaneous Nephrostomy |
| PAs | = Pseudoaneurysms |
| AVFs | = Arteriovenous Fistulas |
| PVA | = Polyvinyl Alcohol |
CONSENT FOR PUBLICATION
Explicit written consent was secured from the patient, as this case report contains no identifiable patient data.
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.
ACKNOWLEDGEMENTS
Declared none.

