All published articles of this journal are available on ScienceDirect.

Thrombocytopenia in Continuous Kidney Replacement Therapy (CKRT): A Systematic Literature Review and Assessment of its Clinical Relevance
Abstract
Introduction
Thrombocytopenia can increase during Continuous Kidney Replacement Therapy (CKRT) in critically ill patients. This is the first systematic review that assesses whether thrombocytopenia during CKRT is clinically relevant.
Methods
The authors comprehensively evaluated CKRT-related thrombocytopenia data. Qualitative and quantitative tools were used to assess quality and risk of bias, epidemiology, causality, clinical outcomes, and possible mitigation and management strategies in the included publications. A subset analysis using Hedges’ g was conducted to assess the impact of the various parameters of interest.
Results
Independent review of over 9,273 records by three authors produced 119 that met the inclusion criteria, and 85 full-text articles involving 29,217 patient samples were evaluated. A descriptive analysis is provided. Most studies were of poor quality (RCTs: 50%; Cohorts: 71%; Systematic Reviews/Meta-analyses: 66%; Cases: 67%). Case studies were fair (67%) to good (33%) quality. The level of certainty of the evidence was moderate for device-related, non-anticoagulant drugs, underlying conditions, and risk factor effects. A high level of evidence certainty was established for anticoagulant drugs, clinical outcomes (mortality/survival, bleeding risk, and filter life), and management and prevention. The subset analysis revealed small to large effect sizes for 19 parameters.
Discussion
While platelet reductions exceeding 40% are associated with increased morbidity, the impact of CKRT on thrombocytopenia was reversible following treatment cessation in many patients.
Conclusion
This systematic review is the first to conclude that CKRT-induced thrombocytopenia appears reversible and may not be clinically significant unless affected by additional risk factors, including medications and existing comorbid conditions.
1. INTRODUCTION
The body’s primary defense against bleeding or hemorrhage involves activating circulating blood cells known as platelets [1]. These cells remain inactive until they detect endothelial damage caused by tumor metastasis, thrombosis, inflammation, wound healing, and atherosclerosis. Platelets adhere to exposed structural proteins like collagen, von Willebrand Factor (vWF), or thrombin, which initiates molecule aggregation and stabilizes the vasculature [2]. Loss of these cells, or thrombocytopenia, typically indicates a decline in platelet levels below the normal range of 150 to 450 x 103/µL [3-5]. However, various definitions are found in the literature, including (1) a percentage reduction in platelets from <30% to >50% with a nadir of >20%; (2) the timing of the decrease in platelet count; (3) the occurrence of thrombosis (new, progressive, or recurrent) or other complications; (4) other causes of thrombocytopenia; and (5) platelet levels falling below 100,000/µL [3, 4]. Thrombocytopenia is also described as either a primary or secondary event.
The diagnosis of thrombocytopenia is typically derived from the patient’s medical history, physical examination, laboratory tests (such as platelet serotonin-release assay, peripheral blood smears, liver and kidney tests), and the 4T score, which includes Thrombocytopenia, the Timing of the onset of thrombocytopenia, Thrombosis or other sequelae, and other causes of thrombocytopenia [6-9].
Disease-related causes for platelet reduction include decreased production from aplastic anemia, myelodysplastic syndromes, and/or increased destruction of platelets due to Disseminated Intravascular Coagulation (DIC) and thrombotic microangiopathies [9]. Eighty percent of all cases are primary, consisting of isolated episodes unrelated to any specific disease. Secondary events may arise from underlying immune disorders, such as Systemic Lupus Erythematosus (SLE), lymphoproliferative disorders, or infections (e.g., HIV), and can also be drug-induced (e.g., linezolid, heparin). Thrombocytopenia affects about 60% of critically ill patients, presenting with varying severities from multiple potential sources, including primary underlying illnesses, comorbidities, and supportive interventions [10, 11]. While significant sources and consequences of thrombocytopenia have been reported, no systematic reviews or definitive guidelines comprehensively evaluate the overall implications of the data on thrombocytopenia during CKRT. This systematic review aims to collate the data and determine whether thrombocytopenia during Continuous Kidney Replacement Therapy (CKRT) is clinically relevant. Please note that Continuous Renal Replacement Therapy (CRRT) is now called CKRT, based on terminology changes made by the KDIGO workgroup in 2020 [12, 13].
2. METHODS
2.1. Literature Search and Selection Criteria
This observational, retrospective analysis was conducted as a systematic review of all relevant literature on thrombocytopenia in CKRT that aimed to determine its clinical relevance. Three independent reviewers conducted systematic literature reviews in PubMed, Google Scholar, and Embase to gather the latest clinical evidence on CKRT/CRRT and thrombocytopenia, covering epidemiology, potential mechanisms and risk factors, clinical outcomes, devices used, anticoagulation, circuit clotting, and possible mitigation and management strategies. Searches focused on English-language literature, specifically human studies limited to adults 18 years and older with acute kidney injury requiring CKRT or Intermittent Hemodialysis (IHD). There were no restrictions on publication year. Eligible studies comprised randomized controlled trials, retrospective and prospective cohort studies, case reports, systematic reviews, meta-analyses, and review articles (Table 1). The specific search and sampling criteria used are detailed in Supplemental Table 1. Studies that did not encompass the defined themes were excluded, including those with pediatric patients and those with missing data. Those meeting the inclusion criteria underwent a full-text review. DAS, NW, and TT evaluated all full-text reviews and reached consensus on the final studies included (N=119; consisting of 15 RCTs, 29 retrospective cohort studies, 20 prospective cohort studies, seven systematic reviews/meta-analyses, 12 case studies, 36 guidelines/expert opinions, and scoping reviews). Figure 1 below illustrates the overall inclusion and exclusion of studies. The quality of the included studies was assessed using the Newcastle–Ottawa Risk of Bias quality assessment. A descriptive analysis of the data is presented.
| Study Design (#) | Total # of Patients (mean ± SD) |
|---|---|
| RCTs (15) | 5972 (373.3 ± 564.9)# |
| Systematic Reviews and Meta-analyses (7) | 5406 (901 ± 679.0) |
| Retrospective Cohort Studies (29) | 8298 (276.6 ± 315.8) |
| Prospective Cohort Studies (20) | 5180 (235.5 ± 494.6) |
| Case Studies (12) | 31 (2.6 ± 3.4) |
| Guidelines/Scoping Reviews (36) | Not reported |
The means ± SD were calculated to determine the subset from which data could be extracted. Depending on the study type comparison, the calculated values for Hedges’ g range from 0.22 to -1.27 standard deviations (Table 2). The effect sizes are small to large.
2.2. Risk and Quality Assessments
Qualitative and quantitative tools were used to assess the included publications. Three investigators assessed the quality of the included studies using the appropriate tools with adjudication of any discrepancies. The Cochrane Risk of Bias (RoB) 2 tool was used to evaluate RCTs as low, unclear, or high quality (Fig. 2A and B) [14]; the Newcastle–Ottawa Risk of Quality assessment forms were used for cohort studies, rated as poor, fair, or good (Fig. 3) [15]. The AMSTAR 2 checklist was used to assess systematic reviews and meta-analyses (critically low, low, moderate, or high) (Fig. 4) [16]. The JBI checklists were used for case studies and scoping reviews (included if the score was yes for 7 of 8 questions) (Fig. 5) [17]. The overall outcomes assessed were the occurrence of thrombocytopenia during CKRT and the recovery from CKRT-induced thrombocytopenia.
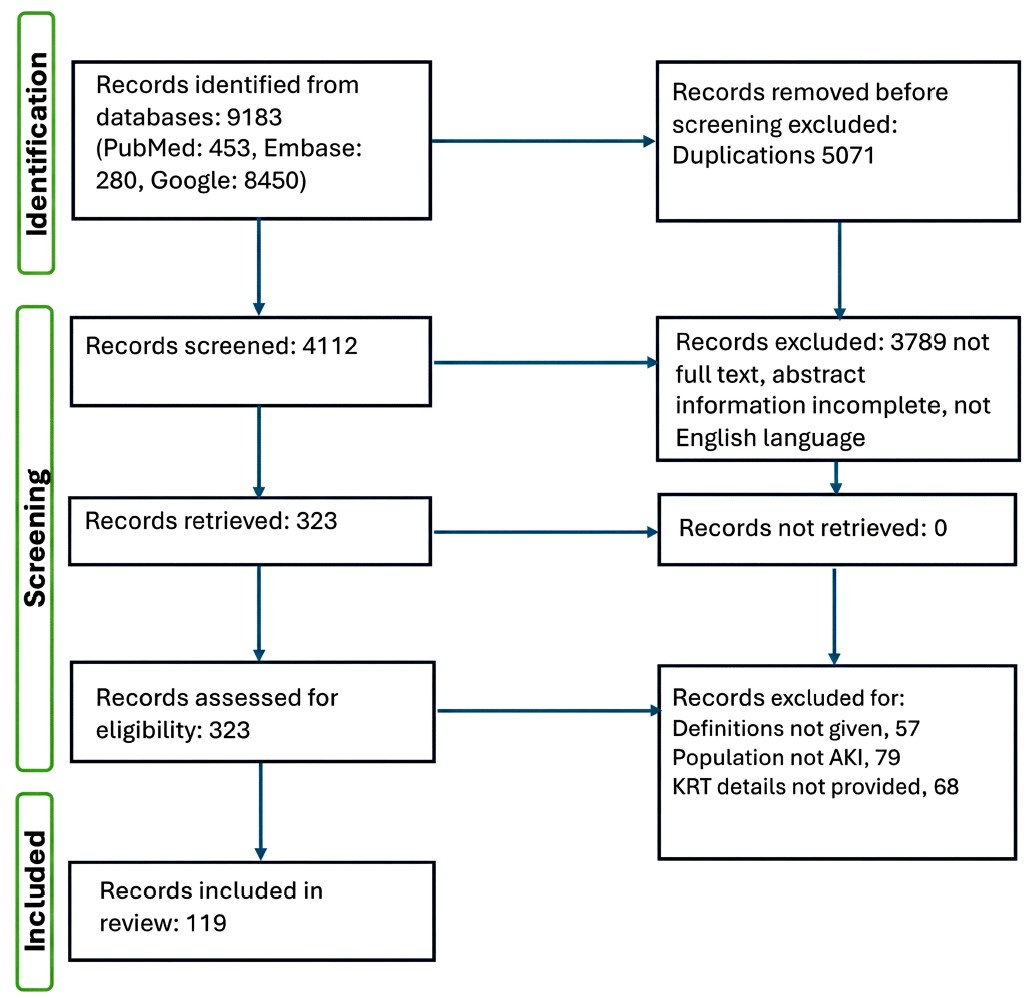
Prisma diagram showing inclusion and exclusion of studies identified from search criteria.
| Group 1 / Group 2 | RCTs | Systematic Reviews / Meta-analyses | Retrospective Cohorts | Prospective Cohorts |
|---|---|---|---|---|
| RCTs | - | - | - | - |
| Systematic Reviews / Meta-analyses | 0.85 | - | - | - |
| Retrospective Cohorts | 0.22 | 1.27 | - | - |
| Prospective Cohorts | 0.26 | 1.12 | 1.04 | - |
| Case Studies | 0.66 | 1.33 | 0.87 | 0.47 |
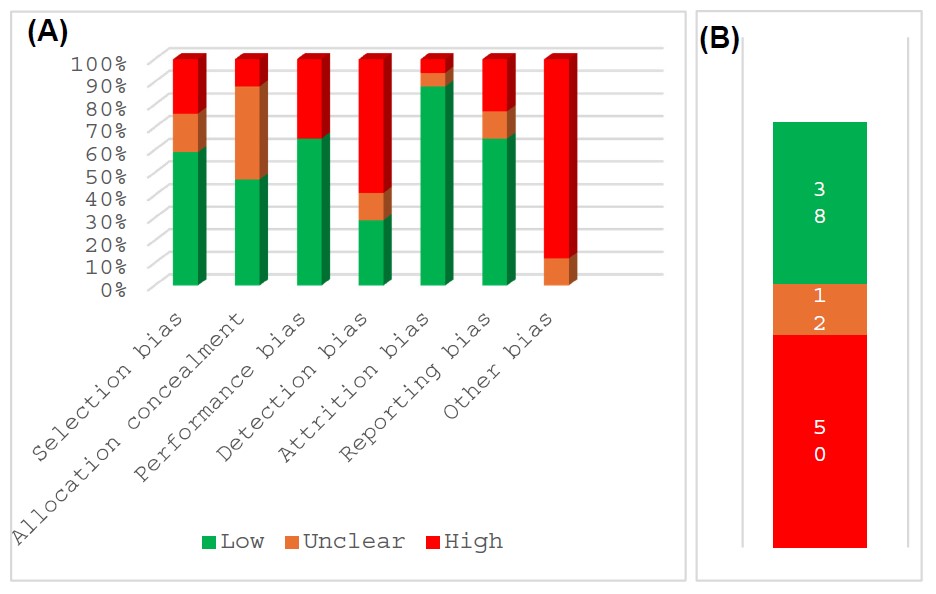
RoB 2 assessment of RCTs.
Legend: (A) The percentages of studies (y-axis) showing low (green), unclear (orange), and high (red) risk of bias are presented here using the cochrane risk of bias (RoB 2) tool. Categories of bias are shown on the x-axis. (B) Percent of studies with overall low (green), unclear (orange), and high (red) risk of bias.
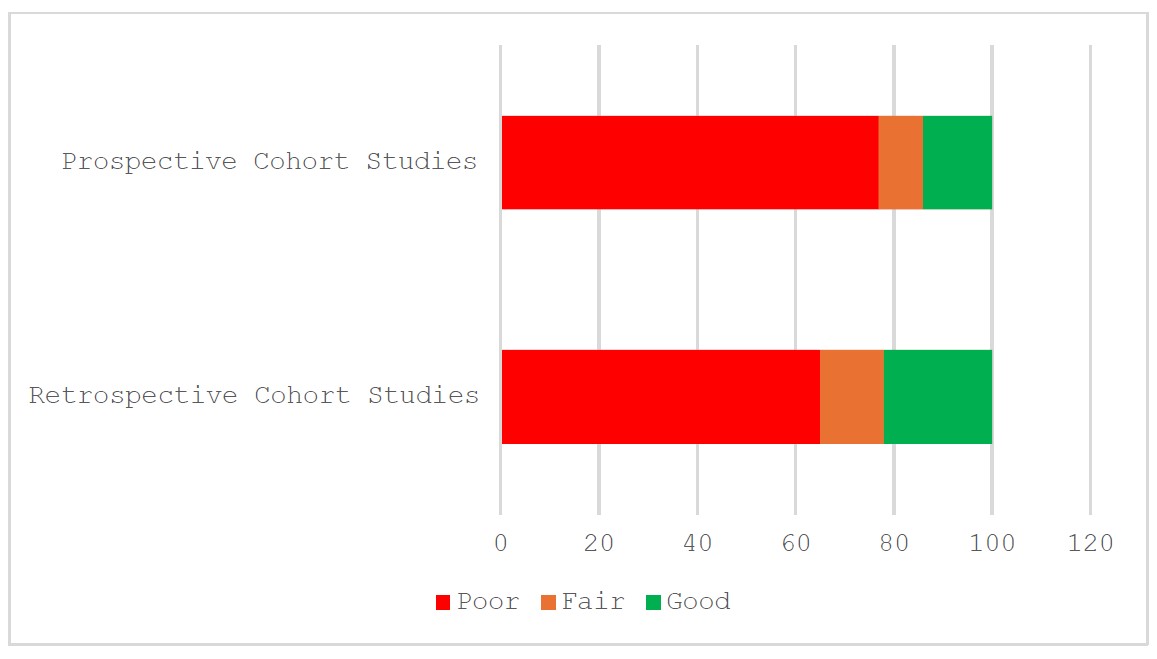
Newcastle assessment of cohort studies.
Legend: Quality of cohort studies assessed using the newcastle assessment tool. The percentages of studies (x-axis) showing good (green), fair (orange), and poor (red) quality are presented here.
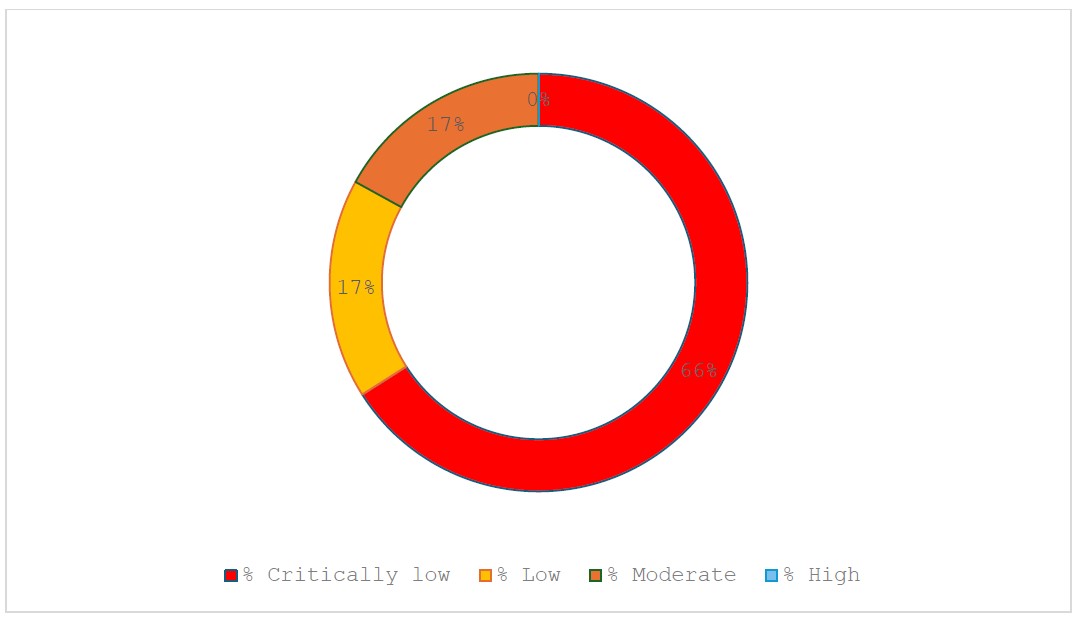
AMSTAR 2 quality assessment of systematic reviews or meta-analyses.
Note: Pie chart representing the quality of systematic reviews and meta-analyses assessed using the AMSTAR 2 assessment tool. Publications were rated as high (green), moderate (orange), low (yellow), and critically low (red).
JBI quality assessment of case studies.
Note: Pie chart representing the quality of case studies assessed using the JBI assessment tool. Publications were rated as good (green) or fair (orange).
Using a subset of 85 studies with 29,217 patients, the five GRADE considerations, the risk of bias, consistency of effect, imprecision, indirectness, and publication bias, were used to summarize the certainty of the body of evidence, graded as high, moderate, low, and very low (Table 2) [18].
2.3. Statistical Analysis
Using Microsoft Excel, we calculated the means and standard deviations for 119 studies to determine different study categories. A subset analysis of 85 studies, excluding reviews and guidelines, was performed to determine the total number of patients for each of 19 parameters. Hedges’ g was used to calculate the effect size by study design and each parameter according to the following (Group 1 vs. Group 2, Tables 3 and 4) [18-21].
Using 85 studies with participant numbers (N=29,217), the mean ± SD was 343.73 ± 583.6. Table 4 shows the calculated values for Hedges’ g for paired parameters. The calculated effect sizes were very small to moderate for 14 parameters and large for five.
| Assessed Parameter, M±SD |
Subgroup: # of Studies; N: # of Patients |
Level of Certainty |
|---|---|---|
| Epidemiology Mean: 347.8 ± 390.1 | 17; N=5913 | Low, due to underlying comorbid conditions, differences in definitions of thrombocytopenia, inconsistent treatment criteria across studies, and variable responses to therapeutic options. |
| Severity Mean: 49.4 ± 40.2 | 6; N=346 | Low, due to underlying comorbid conditions, differences in definitions of thrombocytopenia, inconsistent treatment criteria across studies, and variable responses to therapeutic options. No RCTs, only NRSIs. |
|
Proposed Mechanisms and Potential Risk Factors for CKRT-Associated Thrombocytopenia
Total N=20,724 Overall Mean: 211.5 ± 687 |
Membrane 7 N=808 Mean: 115 ± 281.6 |
Low, due to underlying comorbid conditions, differences in definitions of thrombocytopenia, inconsistent criteria and results across studies, and variable responses to therapeutic options. No RCTs, only NRSIs. |
| Sterilization techniques 7 N=389 Mean: 55.6 ± 47.4) |
Low, due to underlying comorbid conditions, differences in definitions of thrombocytopenia, inconsistent criteria and results across studies, and variable responses to therapeutic options. No RCTs, only NRSIs. | |
| Device-related effects 10 N=4621 Mean: 462.1 ± 1136.5) |
Moderate, upgraded from low due to plausible directional effect. | |
| Flow rates 4 N=742 Mean: 185.5 ± 326.1 |
Low, due to underlying comorbid conditions, differences in definitions of thrombocytopenia, inconsistent criteria and results across studies, and variable responses to therapeutic options. No RCTs, only NRSIs. | |
| Anticoagulant drugs 46 N=9002 Mean: 195.7 ± 530.3 |
High, multiple high-quality studies showing consistency across studies. | |
| Non-anticoagulant drug 7 N=1307 Mean: 186.7 ± 466.3 |
Moderate, upgraded due to directional effect and consistent effect across studies. | |
| Underlying conditions and risk factors 17 N=3855 Mean: 226.8 ± 1027.6 |
Moderate, upgraded due to directional effect and consistent effect across studies. | |
|
Clinical Outcomes
(Total N=12,113) Mean: 448.6 ± 277.17 |
Mortality/ Survival 4 N=4133 Mean: 1033.3 ± 565.1# |
High-quality RCTs, meta-analyses, and cohort studies were included with consistency of effects and low risk of bias. |
| Bleeding Risk 4 N=1226 Mean 306.5 ± 396.3 |
High, good quality RCTs included with consistency of effects, low risk of bias | |
| Infection risk 1 N=797 |
Low, due to imprecision and inconsistency. No RCTs, only NRSI | |
| Kidney recovery 1 N=1508 |
Low, due to imprecision and inconsistency. No RCTs, only NRSIs | |
| Filter/circuit life 9 N=2143 Mean: 238.11 ± 415.7 |
High, low risk of bias, consistency of results | |
| ICU length of stay 1 N=94 |
Low, due to imprecision and inconsistency. No RCTs, only NRSIs | |
| Reversibility 7 N=2712 Mean: 387.4 ± 563.1) |
High, upgraded due to directional effect and consistent effect across studies. | |
|
Management and Prevention
Mean: 294.2 ± 277 |
6; N=1765 | High, low risk of bias |
| Group 1 | Epidemiology | Severity | Proposed Mechanisms | Clinical Outcomes | Management/Prevention | - | - |
|---|---|---|---|---|---|---|---|
| 85 studies N=29,217 |
0. 007 | 0. 51 | 0. 21 | 0. 18 | 0. 08 | - | - |
| Proposed Mechanisms N=20,274 |
Membrane | Sterilization | Device-related | Flow Rated | Anticoagulant | Non-anti-coagulant | Underlying conditions |
| - | 0. 14 | 0. 23 | 0. 32 | 0. 03 | 0. 02 | 0. 04 | 0. 02 |
| Clinical Outcomes N=12,113 |
Mortality | Bleeding | Infection | Kidney recovery | Filter Life | ICU | Revers-ibility |
| - | 1. 57 | 0. 49 | 1. 3 | 4. 1 | 0. 69 | 1. 28 | 0. 18 |
3. RESULTS
3.1. Data Quality and Risk Assessments
Quality assessments were performed using specific, validated tools based on the designs of the studies included. For the RCTs, the overall risk of bias was high or unclear across all the studies (Fig. 2), suggesting low quality. The overall quality of the cohort studies was poor (Fig. 3). Also, no high-quality systematic reviews or meta-analyses were identified.
3.2. Epidemiology of Thrombocytopenia in CKRT
Some studies have reported high rates of thrombocytopenia and fluctuations in platelet levels among critically ill patients following the initiation of Continuous Kidney Replacement Therapy (CKRT). Thrombocytopenia has also been documented in patients undergoing all three primary CKRT modalities: Continuous Venovenous Hemofiltration (CVVH), Continuous Venovenous Hemodialysis (CVVHD), and Continuous Venovenous Hemodiafiltration (CVVHDF) [22-24]. An extensive retrospective analysis (N=595) by Akhoundi et al. indicated an incidence of thrombocytopenia of 40%, with 98.1% of cases utilizing CVVH [25]. Data from a historical cohort study of 541 patients collected over three years by Guru et al. revealed that 65% of patients (N=350) exhibited thrombocytopenia before CKRT initiation, while 20% (N=107) developed new-onset thrombocytopenia after CKRT initiation [26]. In contrast, Griffin et al. noted platelet decreases of 51% in their overall cohort and 50% in those with baseline thrombocytopenia [23], suggesting a new onset incidence rate of 1% (N=1508). Overall estimates of thrombocytopenia vary widely among patients, ranging from 18% to 70% of individuals receiving CKRT in an Intensive Care Unit (ICU) for medical, surgical, cardiovascular, neurological, or burn complications [6, 10, 24, 25, 27-29]. This high variation in incidence may be due to individual patients' underlying comorbid conditions, differences in definitions of thrombocytopenia, inconsistent treatment criteria across studies, and variable responses to therapeutic options.
Heparin-Induced Thrombocytopenia (HIT), caused by a heparin-induced, platelet-activating IgG antibody that binds to the heparin-PF-4 complex at the platelet surface, may also occur with CKRT. Warkentin and Greinacher report rates of HIT incidences between 1% and 5% in treated patients, depending on patients’ parameters (e.g., exposure to surgery, medical needs, pregnancy) and heparin preparations [30]. Warkentin in 2015 further stated that 30-50% of patients with serologically proven HIT develop thrombosis, a rate 12-fold higher than controls [31, 32], and therefore, the frequency of HIT in the critically ill may be around 0.3-0.5%. However, a recent study regarding HIT in intensive care units (ICUs) by Althaus et al. reported an incidence of 3.8% (N=392) using the pretest probability for HIT and two sensitive rapid immunoassays [33]. Granted, the diagnosis of HIT in the ICU is challenging as thrombocytopenia is frequent and multifactorial. In addition, false-positive platelet activation or PF4-dependent assays can skew results [31].
3.3. Severity of Thrombocytopenia in CKRT
Griffin et al. reported that 55% of patients (N=132) who developed thrombocytopenia (defined as platelet reduction by ≥50% from baseline before CKRT) did so within 24 hours and 86% within 48 hours of CKRT initiation [34], using a standard CVVH treatment with 50% pre-filter and 50% post-filter fluid replacement, regional citrate anticoagulation, and a blood flow rate of 200 mL/hr. In a small case series of four patients, Goff et al. reported that all patients experienced a significant drop in platelet count in the first 72 hours following CKRT initiation (Table 5), which improved following CKRT cessation [35]. The modality of CKRT was not stated.
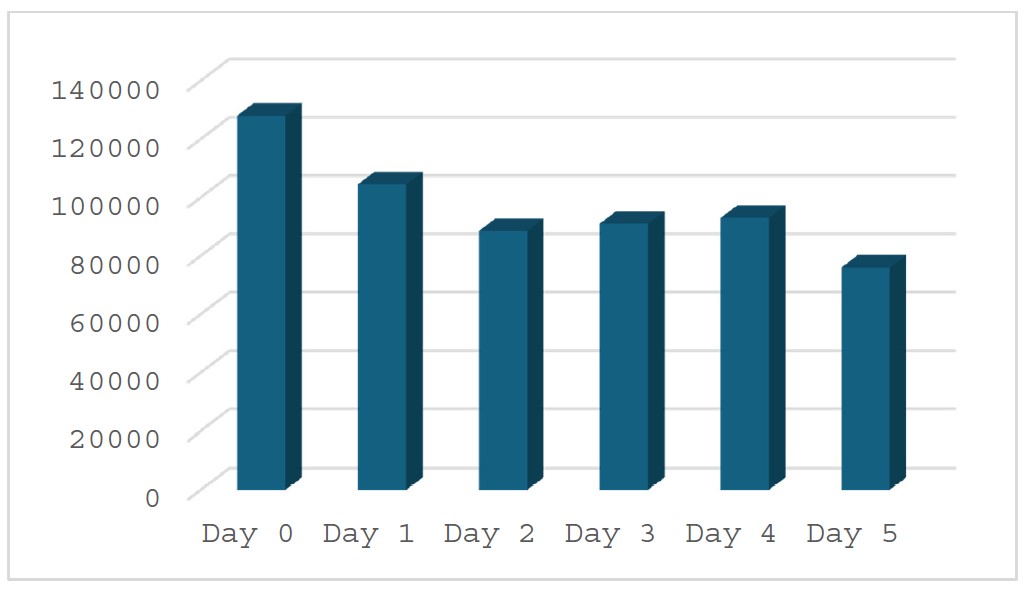
In a study of 33 CVVHDF patients, average baseline platelet counts were 189 x 103/μL and dropped by 31-47% after treatment [22]. Other studies have also reported significant drops in platelet counts for extended periods following initiation of CKRT. A retrospective study by Ferreira et al. [24] evaluated 49 critically ill patients and found an average reduction in platelet count of 47.8%, with platelets reaching their lowest levels at a mean of 4.6 days following CKRT initiation [18]. Platelet levels rebounded following the discontinuation of CKRT, reaching values of > 150 x 103/µL at an average of 2.48 days afterward [24]. Another study by Droege et al. in 80 critically ill adult patients reported overall reductions in median platelet levels over 5 days following CKRT initiation (Fig. 6). The primary modality of use was CVVH (91.3%), followed by CVVHD (5%), or combination therapy CVVH or CVVHD (3.7%) [10].
| Hours since CKRT Initiation | Patient 1: Platelets/µL | Patient 2: Platelets/µL | Patient 3: Platelets/µL | Patient 4: Platelets/µL |
|---|---|---|---|---|
| 0 | 225,000 | 243,000 | 225,000 | 80,000 |
| 24 | 138,000 | 159,000 | 112,000 | 60,000 |
| 48 | 97,000 | 69,000 | 77,000 | 53,000 |
| 72 | 71,000 | 44,000 | 58,000 | 47,000 |
| Hours since CKRT cessation | - | |||
| 0 | 13,000 | 44,000 | 83,000 | 49,000 |
| 24 | 43,000 | 58,000 | 129,000 | 60,000 |
| 48 | 54,000 | 67,000 | 176,000 | 99,000 |
Median platelet counts (per µL).
Much of the published data on thrombocytopenia concerns patients treated with CVVH. However, Brumit and colleagues reported incidences of thrombocytopenia in 57.4% of patients with CVVHD using the NxStage System One and 19.8% of patients (N=147) treated with CVVHDF using the Prismaflex system [36].
3.4. Proposed Mechanisms and Potential Risk Factors for CKRT-associated Thrombocytopenia
The precise mechanism for thrombocytopenia development in patients undergoing CKRT remains an area of active clinical research. Multiple potential explanations and contributing factors, including uremia, sepsis, envenomation, disease severity, mechanical support, shear forces from components of the CKRT circuit (such as the roller pump) or interactions with the hemofilter membrane, method of membrane sterilization, and utilization of heparin or other medications [24, 34, 37-39].
3.5. Membrane Effects
A 2003 study by Mulder et al. evaluated three different machine systems that all used a polyacrylonitrile filter to examine the role of the hemofilter itself inlatelet retention or consumption during CKRT [40]. The study reported a small but significant reduction in mean daily platelet count across the membrane of 2.32 x 109/L, calculating daily platelet loss (with the assumption of continuous operation) of 625 x 109 cells. The authors suggested that a loss of this magnitude in critically ill patients over time could contribute to thrombocytopenia, citing a normal platelet turnover of 120-150 x 109 cells/day and potentially limited capacity for increased platelet regeneration in ICU patients [40]. Blood samples were collected simultaneously from a prefilter (pre-pump) port and a post-filter port, which may obscure the influence of different CKRT circuit components on the emergence of thrombocytopenia [40]. Although unproven, the authors also speculated that the mechanism could be due to platelets' destruction or retention while passing through the circuit's filter or platelet activation.
A review by Daugirdas and Bernardo thoroughly discussed potential causes and the pathophysiology of dialysis-related thrombocytopenia [41]. One possible cause is membrane-triggered complement activation, resulting in thrombocytopenia and neutropenia. Complement activation induces neutropenia and releases neutrophil granules, platelet activation by platelet-activating factor, and decreased platelet counts. Others suggested that polysulfone dialyzer material is considered more biocompatible and causes lower levels of complement activation compared to older membrane types like cuprophan [42, 43]. Daugirdas and Bernardo also reviewed nine non-heparin hemodialysis-associated thrombocytopenia case reports from 1983 to 2011. These reports include the use of dialyzer membranes made from various materials (cuprophan, polyarylethersulfone, polyvinylpyrrolidone, polyamide, and polysulfone) and different sterilization techniques (ethylene oxide, steam, and electron beam). Esteras et al. further concluded that the incidence of hypersensitivity reactions in dialysis patients remains comparable to rates observed over 20 years ago and can occur with all synthetic membranes [44]. They suggest Cellulose Triacetate (CTA) membranes could be a suitable alternative for these patients.
Liu et al. have suggested that the composition of membranes may influence the degree of platelet loss [37]. Patients who underwent CVVH with a CTA membrane, as opposed to a polysulfone membrane, showed no significant decrease in platelet levels [37], indicating that modifying the membrane composition or type might reduce the risk of thrombocytopenia. It is important to note that the CTA membrane has a larger surface area than the polysulfone membrane. Although platelet consumption at the filter could lead to clotting within the circuit, a definitive connection between CKRT circuit clotting and platelet consumption has not been established [45]. Limited evidence from a case report indicated platelet clumping in a CKRT filter, wherein the authors suggested that platelet activation and sequestration within the circuit might account for unexplained thrombocytopenia [40]. Nevertheless, a causal relationship was not determined. According to Joannidis et al., early clotting of filters during CKRT can be attributed to a variety of factors, including the CKRT modality, the circuit itself, the underlying disease burden of the patient, challenges with vascular access, and insufficient biocompatibility [46, 47].
Bonassin et al. retrospectively evaluated the effect of filter surface on clotting and platelet consumption at the membrane in patients in post-dilution CVVHDF with heparin for 7-128 hrs [22]. Using two differently sized filters of the same type, AV 1000S and AV 600S, the investigators observed platelet decreases of 52,000 (range: 0–212,000) in the AV 1000S group and 89,500 (range: 0–258,000) in the AV 600S group (P = 0.64), suggesting that the membrane filter size did not adversely affect thrombocytopenia or clotting.
Ferreira et al. also examined proposed mechanisms for thrombocytopenia in CKRT in their retrospective study of 49 patients treated for 24 hrs using the NxStage System One and the NxStage Purema polyethersulfone membrane. Exclusion criteria included patients with a history of thrombocytopenia and those who required more than two unscheduled filter changes. Due to the latter exclusion, the authors speculated that the cause of the observed thrombocytopenia in their study was not due to loss through clotted hemofilters (i.e., consumption) [24].
Sterilization techniques for dialyzer membranes have been linked to thrombocytopenia in patients undergoing intermittent hemodialysis. Notably, hypersensitivity to Ethylene Oxide (ETO) and electron beam (e-beam) sterilization has been identified as a potential cause of dialyzer-related thrombocytopenia [48, 49]. In a large cohort study by Kiaii et al., post-dialytic thrombocytopenia was observed in patients treated with e-beam sterilized versus non-e-beam sterilized dialyzers [49]. The authors reported that significant thrombocytopenia (a post-dialysis platelet count of less than 100 × 103/µL and a decrease in platelet count of more than 15%) occurred in 7.3% of patients. When switched to non-e-beam sterilized dialyzers, there was a 50% reduction in patients experiencing post-dialysis thrombocytopenia. One randomized crossover study examined platelet activation using PUREMA e-beam-sterilized, Polyethersulfone (PES) dialyzers across various dialysis modes (low-flux HD, high-flux HD, and low- and high-efficiency post-dilution hemodiafiltration or HDF). Platelet activation during these modalities was assessed as low and primarily influenced by anticoagulation [50]. A small but significant decrease in platelet counts was found between high-flux HD and low-efficiency HDF (8 vs. 16%). However, platelet counts remained within normal limits [50]. A more recent case series investigating thrombocytopenia in 28 patients undergoing hemodialysis with the NxStage System One noted the emergence of thrombocytopenia associated with gamma-sterilized PES PUREMA membranes, which were subsequently replaced with steam-sterilized polysulfone membranes [51]. Platelet counts returned to normal following the transition to the steam-sterilized polysulfone membrane. The authors expressed uncertainty regarding the cause of thrombocytopenia, highlighting the need for further investigation [51]. Conversely, subsequent studies indicated no relationship between sterilization techniques and thrombocytopenia [52-54].
3.6. Device-related Effects
Similar reports of decreased platelets (<100 x 103/μL) have been documented in patients on other extracorporeal membrane therapies such as conventional Intermittent Hemodialysis (IHD), Prolonged Intermittent Kidney Replacement Therapy (PIKRT), Cardiopulmonary Bypass (CPB), and Extracorporeal Membrane Oxygenation (ECMO), suggesting a general impact from these types of devices [41, 55-60]. Therefore, thrombocytopenia is not unique to CKRT. Published data also showed that HIT could be observed in patients on mechanical circulatory support devices, with frequencies from 5.3% in non-durable vs. 2.9% in durable ones and 1.3% in the preimplantation settings (P = 0.26) [61].
3.7. Flow Rates
Some studies have associated circuit flow rates with thrombocytopenia, but these findings have not been consistently demonstrated or established as causative for thrombocytopenia and may depend on individual patients [24]. For example, Liu et al. and Mulder et al. reported blood flow rates of 200-250 mL/min and dialysate flow rates of 3 L/hr for all hemofilters utilized [37, 40]. Mulder et al. [40] identified a strong correlation between blood flow rate and the extent of platelet loss, observing a decrease in platelets of 0.07 x 109/L for every mL/min increase in blood flow (p = 0.015), suggesting that higher blood flows were linked to less platelet reduction across the hemofilter compared to lower flows. The authors also speculated that this might be attributed to faster transit time, reduced hemoconcentration, or enhanced rheology. In contrast, Liu et al. [37], did not find flow rates to be implicated in the occurrence of thrombocytopenia. In a retrospective analysis, Brumit et al. reported a higher incidence of thrombocytopenia in cardiovascular ICU patients treated with CVVHD using the NxStage system (35/52) compared to CVVHDF with the Prismaflex system (17/52) [36]. Notably, the average blood flow rate was greater with the NxStage System One (255 mL/hr vs. 200 mL/hr; P < 0.001).
In a retrospective study of 119 patients undergoing CKRT, Harada et al. applied a blood flow rate of 100 mL/min and a mean dialysate flow rate of 492 mL/h in patients requiring CVVHDF (filtration was 206 mL/hr, and ultrafiltration was 12 mL/hr) or 621 mL/h in CVVHD (ultrafiltration was 28 mL/hr) [62]. Decreased blood flow rates were noted in 52 (43.7%) patients and demonstrated no significant impact on clinical parameters, including clotting times; granted, the majority were prescribed CVVHDF vs. CVVHD (100 vs. 19). Ferreira et al. also reported the use of higher blood flow rates of 325 mL/min and lower average dialysate flows at 2.75 L/hr but with no effect of flow rates on thrombocytopenia [24, 37, 40].
3.8. Anticoagulant Drugs
Thrombocytopenia was also observed in patients receiving heparin and non-heparin anticoagulation for CKRT [63]. However, the use of heparin may elevate the risk of bleeding and thrombocytopenia during CKRT [64]. For example, in a small study involving 61 critically ill COVID-19 patients, 13 out of 16 patients (81.3%) on CKRT with heparin as the anticoagulant developed thrombocytopenia, with a platelet count dropping to <50 × 109/L [65]. This contrasted with 12 out of 45 patients (26.7%) who were not on CKRT and one non-ICU patient (1.1%) who also developed thrombocytopenia. Such decreases in platelet count may be more pronounced in severely affected COVID-19 patients with pneumonia, and the authors recommend considering an alternative anticoagulant. The study also suggested that the patient's underlying condition contributes to thrombocytopenia.
Although relatively uncommon in critically ill patients, identifying HIT among cases of non-HIT presents a challenge in the ICU. According to Warkentin, HIT in the ICU should be regarded as a “clinical-pathological syndrome,” where the patient shows symptoms of HIT with plasma containing heparin-induced antibodies, a 4T score of at least 4, and a positive serotonin-release assay test [31]. However, applying the 4T score may not be practical for several reasons. For instance, only 10% of patients with HIT have platelet nadirs <20 x109/L (First T, 2 pts via 4T score). Therefore, platelet decreases would not effectively distinguish HIT from non-HIT unless severe, regarding the second T, when critically ill patients are admitted to the ICU, whether post-surgery or due to acute illness, early-onset thrombocytopenia is expected, which may complicate any HIT diagnosis resulting from subsequent treatments. Postoperative HIT tends to follow a pattern with heparin exposure before the actual onset of HIT. Prior exposure includes early-onset thrombocytopenia, a non-HIT platelet nadir before the detection of heparin/PF4 autoantibodies, the observation of HIT-associated drops in platelet counts, a progressive decline to >50%, and symptomatic thrombosis [66]. Supporting this, platelet counts have been shown to decrease during days 5 and 10 after the initial or re-exposure to heparin [67]. HIT-associated thrombosis (Third T) typically occurs around post-exposure day 10 (median), but the range can be broad, as many patients develop symptomatic thrombosis at various times throughout the episode. To further complicate matters, the ICU abounds with potential “other” (fourth T) causes of thrombocytopenia that are challenging to differentiate, including HIT mimickers such as septicemia, coagulopathies, or antiphospholipid syndromes. Additionally, approximately 10-20% of patients with HIT will develop decompensated disseminated intravascular coagulopathy [31]. Therefore, preventing HIT in the ICU through alternative anticoagulants such as LMWH and nonheparin alternatives like citrate or Direct Thrombin Inhibitors (DTIs) is essential.
A Cochrane review by Tsujimoto et al. involving 34 studies and 1,960 subjects assessed primary outcomes, including major bleeding, successful prevention of clotting, and death associated with the anticoagulant used in CKRT. They reported that, compared to unfractionated heparin, citrate as an anticoagulant may reduce thrombocytopenia (RR 0.39, 95% CI 0.14-1.03) [68]. However, the authors cautioned that this finding has low certainty of evidence, based on three studies with 412 participants [69-71]. The review also indicated uncertainty regarding whether citrate reduces thrombocytopenia compared to low molecular weight heparin, as well as whether Low Molecular Weight Heparin (LMWH) decreases thrombocytopenia compared to unfractionated heparin (UFH) [68]. Other publications have reported a lower incidence of HIT with LMWH than unfractionated heparin [72-76]. One study included patients receiving CVVHD and/or CVVH, but causation could not be established [24]. Liu et al. observed a greater degree of platelet loss in patients undergoing CVVH with polysulfone membranes and no anticoagulation compared to those who received anticoagulation with LMWH after 12 hours of treatment; however, no differences were noted at 6 hours [37].
Furthermore, LMWHs have been linked to reduced metabolic effects, antithrombin affinity, activation of polymorphonuclear cells and platelets, and platelet factor-4 (PF-4), along with higher and more consistent bioavailability [77-80]. It is essential to note that protamine infusion, used to inhibit post-filter heparin, is also associated with several complications, including thrombocytopenia and leukopenia [81].
For patients with HIT, all heparin therapy should be stopped immediately and replaced with heparin locks or non-heparin anticoagulants, such as argatroban (preferred for kidney impairment) or bivalirudin. After medication adjustments, the activated Partial Thromboplastin Time (APTT) should be monitored every four hours and then daily once the target (1.5 to 3.0 times the baseline) has been achieved for two consecutive times [82]. Several case reports indicate that patients refractory to standard HIT treatment can benefit from receiving Intravenous Immunoglobulins (IVIG). However, platelet transfusions should be avoided, as they may increase the risk of thrombosis [83].
In a small crossover randomized study, Opatrný et al. demonstrated that patients on CVVHDF exhibited hemostasis involving thrombocytes, coagulation, and fibrinolysis, with no beneficial effect of heparin rinse on thrombogenicity, complement activation, or blood leukocyte counts [84]. Consequently, the Kidney Disease Improving Global Outcomes (KDIGO) working group recommended citrate as the first-line anticoagulant for CKRT in 2012, while Dickie and colleagues proposed a revised heparin protocol [85-87]. Numerous protocols for effective Regional Citrate Anticoagulation (RCA) have been established. Tolwni et al. recommend using a 2% trisodium citrate solution (citrate 70 mmol/L, sodium 210 mmol/L) in dextrose, infused pre-filter at a rate of 250 mL/hr to maintain a post-filter ionized calcium level of 0.25 to 0.5 mmol/L [88].
Tobe et al. also proposed using an anticoagulant citrate dextrose solution that contains trisodium citrate at 74.8 mmol/L, citric acid at 38 mmol/L, and dextrose at 123.6 mmol/L [89]. A modification of this protocol was suggested by Davies et al. [90] in which a 0.5% citrate concentrate serves as the replacement fluid, and a bicarbonate-based, calcium-free solution is utilized as the dialysate in the application of pre-dilution CVVHDF [87]. In the Berlin protocol, 4% trisodium citrate (408 mmol/L) is diluted and infused at 180 mL/hr (i.e., 136 mmol citrate/L) to achieve a post-filter ionized calcium level of 0.25-0.35 mmol/L. Calcium replacement is administered via calcium chloride, aiming for a systemic calcium concentration of 1.0-1.12 mmol/L [47, 90-92]. Prismocitrate solutions 10/2 (10 mmol/L citrate/2 mmol/L citric acid; 0.336% citrate) and 18/0 (18 mmol/L citrate; 0.529% sodium citrate), as well as anticoagulant citrate dextrose solution-A (ACD-A: trisodium citrate 74.8 mmol/L, citric acid 38 mmol/L, and dextrose 123.6 mmol/L; 3% citrate) have also been used by several investigators [93-98].
Regarding citrate, a meta-analysis by Li et al. reported that the risk of thrombocytopenia was 45% lower with RCA than with heparin [84]. However, thromboprophylaxis is recommended if citrate anticoagulation is utilized in cases of HIT [47, 99].
The ongoing CoV-Hep randomized controlled study aims to assess heparin versus citrate for anticoagulation in CKRT [99, 100]. The study is ongoing in Brazil and includes all ICU patients at the University of São Paulo General Hospital. The primary outcome is the percentage of clotted dialyzers within 72 hours in each studied group. Secondary outcomes include the number of dialyzers used during the first 72 hours of the dialysis protocol, the mortality rate within the first 72 hours of the dialysis protocol, bleeding events (major or minor) in the first 72 hours of the dialysis protocol, the proportion of severe thrombocytopenia (less than 50,000 platelets) within the first 72 hours of the dialysis protocol, dialysis efficiency (variation in urea sieving between the first, second, and third days of the dialysis protocol), CKRT pressures (arterial, venous, dialysate, and pre-filter pressure) during the first 72 hours of the dialysis protocol, and in-hospital mortality. The results are eagerly awaited.
Regarding DTIs, argatroban and bivalirudin have been approved as anticoagulants in the US for adult patients with or at risk for HIT undergoing Percutaneous Coronary Intervention (PCI) [101]. However, their use in CKRT remains off-label. A prospective, dose-finding study conducted in two ICUs with 30 patients revealed that a loading dose of 100 µg/kg of argatroban followed by a steady-state infusion (µg/kg/min) maintained blood urea nitrogen levels at 32.16 ± 18.02 mg/dL and ensured mean filter patency at 24 hours of 98% [102]. Only two patients experienced minor bleeding, with no severe bleeding episodes. In another study involving 80 patients on ECLS, CKRT, or no ECLS, an initial argatroban dose of 0.3-0.5 µg/kg/min successfully achieved therapeutic APTT levels [103]. A recent review by Bachler et al. further recommended using DTIs in septic or COVID-19 patients with confirmed or suspected HIT, HIT-like conditions, impaired fibrinolysis, or those on extracorporeal circuits who show heparin resistance [104]. As for bivalirudin, Tsu et al. retrospectively analyzed its effects in 135 patients with HIT; 5ere on CKRT, 12 on SLEDD, and 24 on IHD [105]. Patients on KRTs required dose reductions (0.07, 0.09, and 0.07 mg/kg/h) compared to those with normal kidney function, but had higher dosing needs than CKD stage 4 or 5 patients not on KRTs. This aligns with findings from Runyan et al. in patients treated with CVVH [106].
The use of prostaglandins to inhibit platelet activation may also be considered, as heparin can lead to platelet activation [107]. Significant drawbacks for routine use include their high costs and hypotension due to vasodilation, although the half-life of the vasodilatory effect is as short as 2 minutes. In a retrospective report involving 248 patients, 38 (15%) received prostacyclin as an anticoagulant for more than 72 hours [108]. Epoprostenol was indicated due to filter hypercoagulability in 48%, thrombocytopenia in 68%, and hemorrhage in 3% of cases [109].
Administering aspirin and antiplatelet inhibitors may reduce the rates of thrombocytopenia with CVVHDF in patients with normal platelet counts at baseline [36, 110-114].
3.9. Non-anticoagulant Drugs
Interestingly, a case report suggests that the use of flucytosine may increase the risk of thrombocytopenia in critically ill patients on CKRT [115]. The initial differential diagnosis and assessment included inflammatory pneumonitis, infection, and immunologic pathology. The patient was ultimately placed on intermittent hemodialysis three times a week and received flucytosine at a dose of 2,500 mg on dialysis days. On hospital day 27, the patient began CVVH due to hemodynamic instability and baseline thrombocytopenia (39 × 103/μL); multiple vasopressors were also added to the treatment regimen. The dose of flucytosine was increased to 2,500 mg every 12 hours. Over 72 hours of CVVH, the patient had a mean urine output of approximately 0.21 mL/kg/day and was classified as experiencing nonoliguric kidney failure. Flucytosine was discontinued on hospital day 29 due to thrombocytopenia, and high-dose fluconazole was introduced. The nadir platelet count was 15 × 103/μL on hospital day 31, nine days after starting flucytosine. It has been suggested that targeting flucytosine trough levels of 25-100 μg/mL may be beneficial, as higher levels have been linked to an increased incidence of thrombocytopenia and elevated liver enzymes. The patient’s flucytosine peak and trough levels were 120 μg/mL and 81 μg/mL, respectively. Pharmacokinetic calculations indicated an elimination rate constant (ke) of 0.04/hr, with a half-life (t1/2) of 16.75 hours. The total clearance was 1,924-2,308 mL/hr (range based on 75-90% bioavailability) and was lower than expected. This resulted in significant hematologic toxicities, prompting the discontinuation of the drug. Unfortunately, the patient passed away.
Other medications, such as NSAIDs, quinine, antiarrhythmics, and antiepileptic drugs, can also lead to thrombocytopenia (Supplemental Tables 2-5) [64, 116-120]. Risk factors contributing to the development of thrombocytopenia due to medications like linezolid include the duration of therapy, kidney impairment, the concurrent use of kidney replacement therapies, and the administration of unfractionated heparin (P <0.05 for all) [121, 122]. Coagulation issues arising from coagulation disorders or inadequate anticoagulation have also been linked to higher rates of thrombocytopenia [24]. Therefore, a comprehensive patient assessment and medical history should be conducted upon ICU admission.
The focus of treating drug-induced thrombocytopenia in critically ill patients is to eliminate or control the cause as quickly as possible. The initial step for drug-induced thrombocytopenia is the immediate discontinuation of the offending agent(s). Nevertheless, the risks versus benefits of discontinuing the drug should be evaluated, along with the availability and effectiveness of alternative treatments. If the risks associated with thrombocytopenia outweigh those of discontinuing the drug, then the drug should be promptly discontinued or substituted with a medication that has a different chemical structure. In addition to stopping the offending medication, platelet transfusions may be initiated for symptomatic or high-risk patients, except for those with HIT. Corticosteroids, IVIG, and plasmapheresis may also be beneficial, though their use is limited mainly to case reports or case series. Platelet growth factors do not have a role in managing drug-induced thrombocytopenia [83].
Glucocorticoids can be used for immune thrombocytopenia and thrombotic thrombocytopenic purpura. They inhibit the production of the autoantibody IgG, stabilize platelets and the endothelial cell membrane, reduce the destruction of platelets and red blood cells, and stimulate hematopoiesis in the bone marrow. Intravenous Immunoglobulin (IVIG) and monoclonal antibody drugs are alternative options for immune thrombocytopenia. IVIG acts faster than glucocorticoids and is often utilized to treat immune thrombocytopenia with significant bleeding in patients requiring emergency invasive surgery and in refractory cases of immune thrombocytopenia. The combination of IVIG and plasma exchange is regarded as a treatment option for resistant cases. Additionally, high-dose IVIG may be effective for Heparin-Induced Thrombocytopenia (HIT) that does not respond to conventional anticoagulation therapy [82].
In cases of drug-induced immune thrombocytopenia, platelet counts generally recover after 4 to 5 half-lives of the offending agent. Administering platelets before the drug has been fully cleared from the system may not be adequate. Nonetheless, this approach should be considered in instances of severe bleeding. For patients with significant thrombocytopenia and bleeding or those at high risk for bleeding, high doses of IVIG, such as 1 g/kg of body weight, may be given to facilitate rapid platelet recovery [123].
Concerning drug-induced thrombocytopenia resulting from immune checkpoint inhibitors (monoclonal antibodies utilized in cancer treatment targeting the proteins PD-L1 and CTLA4), the American Society of Clinical Oncology recommends management according to platelet count, classified by grade [110]. Thrombocytopenia classified as Grade 1 (platelets < 100x109/L/L) and Grade 2 (platelets < 75x109/L/L) should be managed by continuing therapy along with rigorous laboratory evaluation and follow-up. However, if the platelet count fails to improve or continues to decline, therapy should be paused. For Grades 3 and 4 (platelets <50x109 /L), consulting a hematologist is advised, and treatment should be withheld. Management should include high-dose corticosteroids and/or IVIG for a minimum of four weeks, and if thrombocytopenia persists, infliximab may be considered. For patients who do not experience improvement, alternative treatments such as rituximab or thrombopoietin receptor agonists can be employed. If the patient cannot recover to at least Grade 1, immune therapy should not be resumed [123].
Platelets typically recover quickly after discontinuing eptifibatide and tirofibor in patients with glycoprotein (GPIIb/IIIa) inhibitor-induced thrombocytopenia. However, since abciximab is an irreversible platelet aggregation inhibitor, recovery may take 2 to 5 days following cessation. Along with stopping the GPIIb/IIIa inhibitor, discontinuing anticoagulants and antiplatelets might also be necessary. In cases of significant bleeding, platelet transfusions may be administered. Limited data regarding corticosteroids or IVIG for GPIIb/IIIa inhibitor-induced thrombocytopenia are available [83].
Regarding antibiotic-induced thrombocytopenia, experts recommend that antibiotic therapy for treating sepsis or septic shock should be sustained due to the heightened risk of mortality associated with delayed or inadequate treatment, while closely monitoring the platelet count. The risks of discontinuing the antibiotic and the availability of alternative effective antibiotics should be carefully evaluated for other infections. Concerning linezolid, a retrospective observational study involving 102 patients found that thrombocytopenia occurred in 17.6% of patients treated with linezolid for an average of 14 days [122]. Although linezolid-induced thrombocytopenia may resolve after discontinuation and treatment with pyridoxine, this approach may not be widely applicable, as only 2 case reports have shown benefit. Additionally, for trimethoprim/sulfamethoxazole, one case report described the effective management of drug-induced thrombocytopenia after the drug was discontinued and following the administration of 2 units of platelets and oral prednisone. In another case report, a patient’s trimethoprim/sulfamethoxazole-induced thrombocytopenia resolved two weeks after the drug was discontinued, and prednisone was initiated at a dosage of 1 mg/kg daily [83].
Depending on the specific medication, potential management for antiepileptic drug-induced thrombocytopenia in critically ill patients varies. Thrombocytopenia resulting from valproic acid usually develops several months after starting treatment and may improve after dosage reduction. Discontinuation is not always required. In contrast, thrombocytopenia associated with phenytoin is believed to be immune-mediated, so discontinuation of the drug is recommended. Furthermore, in case reports, platelet transfusions may not be effective, but there might be advantages linked to the use of IVIG [83].
Desmopressin (DDAVP) can improve platelet function in patients taking antiplatelet medications. It promotes the release of von Willebrand Factor (vWF) and factor VII, enhances platelet adhesion and aggregation, and is the preferred treatment for bleeding related to von Willebrand Disease (vWD). DDAVP has demonstrated effectiveness in improving platelet aggregation in patients using aspirin and/or clopidogrel and in reducing postoperative bleeding in cardiac patients [82].
3.10. Underlying Conditions and Risk Factors
Sepsis is described in the medical literature as one of the most common risk factors for the development of thrombocytopenia in ICU patients [5]. Critically ill septic patients may be more susceptible to thrombocytopenia following the initiation of CKRT. A retrospective cohort study by Fay et al. evaluated 160 septic patients, comparing rates of thrombocytopenia between those who received KRT, CVVH, or Accelerated Venovenous Hemofiltration (AVVH) and those who did not [124]. The incidence of thrombocytopenia within the first 5 days of hospitalization was more than ten times greater among septic patients receiving KRT compared to those who did not receive such support (67.5% versus 6.3%, P < 0.001) [124]. Patients supported with CVVH had a higher rate of thrombocytopenia than those supported with AVVH (76% versus 53.3%, P = 0.049) [124]. However, causality could not be established due to the study's retrospective nature, although the authors noted an association between increased KRT exposure and thrombocytopenia. Since some patients in this study experienced a delayed onset of thrombocytopenia, the authors suggested that clinicians managing septic patients requiring KRT should consider extending monitoring for thrombocytopenia in this population due to the potential for later presentation [124].
Not all studies have reported increased rates of thrombocytopenia in septic patients following CKRT initiation. A retrospective study by Droege et al. involving 80 critically ill adults assessed the change in platelet count within patients after starting CKRT therapy using heparin as the anticoagulant over 5 days [10]. They found that patients who were septic at the time of CKRT initiation had a lower rate of thrombocytopenia at day 3 compared to non-septic patients (42.9% vs. 68.1%, P = 0.033), with overall rates of thrombocytopenia being similar between the two groups [10]. The median platelet count at CKRT initiation was 128,000/µL. Serial decreases in platelet counts were noted on days 1-5. Twenty-five (35%) patients exhibited thrombocytopenia at the start of CKRT compared with day 2 (56.3%), day 3 (58.7%), and day 5 (59.1%) (P < 0.05 for all). One patient was diagnosed with HIT. While the authors of this study did not explain this finding, other publications have speculated that CKRT might improve thrombocytopenia in septic patients by clearing inflammatory mediators, assuming they are small enough to pass through the filter’s pores [125].
Limited data from patients undergoing cardiac surgery suggest that acute disturbances in microcirculation perfusion may persist after the surgery, leading to microthrombi formation and platelet dysfunction [126, 127]. Some authors speculate that these effects might precipitate ischemic injury in the kidney, and microthrombi formation could be linked to kidney failure [128].
In a retrospective analysis of 125 patients who received continuous venovenous hemofiltration (CVVH), Wu et al. identified female gender, older patient age, and a longer disease course as risk factors for significant reductions in platelet values [125]. The use of CVVH for 3 days resulted in 44.8% and 16% of patients experiencing mild declines (20–49.9%) and severe declines (≥50%) in platelet count, respectively; 37.6% and 16.0% of patients exhibited mild thrombocytopenia (platelet count 50.1–100 x 10^9/L) and severe thrombocytopenia (platelet count ≤50 x 109/L), respectively. However, using multivariate logistic regression, Droege et al. found that age, gender, heparin infusion, CKRT circuit clotting, surgical ICU setting, and exposure to β-lactam antibiotics were not associated with thrombocytopenia in critically ill patients receiving CKRT [10]. Nonetheless, CKRT circuit clotting had a non-significantly associated odds ratio (OR) of 1.08 (95% CI 0.353-3.309). Only the Sequential Organ Failure Assessment (SOFA) Score at the time of CKRT initiation was identified as a risk factor for thrombocytopenia in critically ill patients (OR 1.22; 95% CI = 1.041-1.439), with the critical caveat that the multivariate analysis was likely underpowered due to the low number of thrombocytopenia cases [10].
In a secondary analysis of the Randomized Evaluation of Normal versus Augmented Level (RENAL) Study, a higher percentage of patients with reduced platelets were females (36.6% vs. 23.7%, P = 0.0005). These patients had elevated Acute Physiology and Chronic Health Evaluation (APACHE) III scores (101.6 vs. 91.5, P < 0.0001), a greater incidence of sepsis (50.3% vs. 38.4%, P = 0.002), and higher international normalized ratio (INR) values (1.7 vs. 1.5, P < 0.0001) at baseline compared to those without platelet drops [39]. Higher SOFA coagulation scores at baseline were also linked to lower platelet counts. Elevated SOFA scores were also observed in CVVHD patients with greater thrombocytopenia [36].
A single-center, case-control observational study involving 795 patients and over 166,950 hours of delivered CKRT at Johns Hopkins Hospital reported a higher incidence of thrombocytopenia in the Cardiac Intensive Care Unit (CICU) compared to the medical ICU (MICU; 22.5% vs. 13.1%) at 72 hours [34]. Concurrent thrombocytopenia in patients receiving CKRT was defined as a decrease in platelet count of ≥50% within 72 hours of therapy initiation. Using logistic regression, the study also reported that the unadjusted and adjusted odds ratios for developing thrombocytopenia were more than twice as high in the CICU compared to the MICU. The time to the thrombocytopenia episode was also longer in the CICU than in the MICU (29 vs. 17 hours). The authors speculated that their patients' long duration of CKRT (219 hours) may have contributed to thrombocytopenia, though most patients demonstrated this effect at 48 hours (86%). While still not entirely clear, the authors suggested that a higher rate of congestive heart failure, coronary artery disease, and aspirin use in CICU patients compared to those in the MICU, along with differences in disease management, could explain the discrepancies in incidences.
It is unclear whether platelet rebound results from the overall improvement in disease severity after CKRT or the cessation of CKRT itself. Interestingly, Ferreira reported that 12% of patients recovered during therapy, suggesting that factors beyond CKRT are involved [24]. Data on platelet rebound during CKRT is limited, but one potential reason for reactivating the coagulation cascade could be the withdrawal of thromboprophylaxis or the anticoagulant medication [129, 130].
In some situations, CKRT has been shown to relieve conditions that cause thrombocytopenia. For example, HELLP syndrome is a rare but serious pregnancy complication characterized by hemolytic anemia, elevated liver enzymes, and low platelet counts (thrombocytopenia) [131]. A case report involving a 27-year-old pregnant woman with HELLP syndrome who developed respiratory failure and urine output below 100 mL/hr noted that early continuous venovenous hemofiltration and nitric oxide therapy enabled the patient to improve clinically and eventually be discharged [132]. Another similar report was documented [133]. Additionally, a case involving a pregnant woman with hemorrhagic fever who presented with thrombocytopenia, among other conditions, reported successful CKRT treatment, leading to full recovery after 21 days, with a healthy delivery and 1-year follow-up [134]. CKRT, combined with a novel cytokine adsorption therapy, was also successfully utilized to treat a case of septic shock with thrombocytopenia due to β-hemolytic streptococcus-induced necrotizing fasciitis. In another instance, a 38-year-old Chinese female with alcohol-induced acute pancreatitis complicated by HUS and a steady decline in kidney function over 2 days received daily CKRT for a total of 13 treatments [135]. She also had intermittent transfusions of fresh frozen plasma. Her kidney failure was effectively addressed, resulting in the return of normal kidney function.
3.11. Clinical Outcomes
3.11.1. Mortality/Survival
Mortality has also been associated with the severity of thrombocytopenia in patients receiving CKRT. Wu et al. reported that patients receiving CVVH over 3 days who showed a ≥50% decline in platelet count faced a higher mortality risk compared to those with milder platelet reductions (35.0% survival versus 59.0% survival, P = 0.012) [125]. However, patients with severe thrombocytopenia overall had a survival rate comparable to those without severe thrombocytopenia (45.0% versus 57.1%, P = 0.308), indicating that a significant drop in platelet counts was not an independent mortality risk factor, based on a multivariate-adjusted Cox regression model. They speculated that this might be due to bone marrow dysfunction or other causes of platelet destruction unrelated to CKRT.
A post hoc analysis of the Acute Renal Failure Trial Network (ATN, N=1,124) Study compared outcomes of thrombocytopenia among patients receiving IHD or CKRT. It reported that CKRT was not an independent predictor of worsening thrombocytopenia compared to IHD. Patient survival stood at 87.9% (N = 989) after a minimum of 48 hours of KRT [136]. Patients who exhibited changes in platelet counts following KRT initiation were classified based on those with platelet increases or decreases. Since very few patients had platelet values exceeding 150 × 103/μL at baseline, a normal platelet count was set above 100 × 103/μL. In comparison, a low platelet count was identified when values fell below 100 × 103/μL. Among the survivors, 619 patients (63%) experienced an average decrease in platelet count of 33% after KRT initiation, and 139 patients (14%) had at least a 50% reduction in platelet numbers from baseline. Fifty-two percent of patients showed typical platelet values at baseline, and 67% of those who survived beyond the 48-hour point of KRT had approximately a 30% reduction in platelet levels.
Severe reductions in platelet count (>50%) in critically ill patients beginning CKRT can be problematic. One study abstract reported that CKRT patients with a significant drop in platelet count were more than three times more likely to die in the hospital than CKRT patients who saw an increase in platelet count from baseline [137]. Their findings support Guru et al., indicating that preexisting thrombocytopenia and new-onset thrombocytopenia before CKRT were significantly associated with increased ICU mortality [26]. Additionally, Griffin et al. concluded that although a decreased platelet count during CKRT was significantly linked to 60-day mortality, it did not affect 28-day or 1-year mortality. This suggests that CKRT is not an independent predictor of worsening thrombocytopenia compared to those treated with intermittent hemodialysis [136].
Lin et al. assessed point-of-care parameters, including survival and platelet counts, in 1,454 patients with complete datasets [45]. Survival after four days was 81%, with 83.2% of these patients experiencing reduced platelet counts. The mean daily platelet count was 230 × 109/L throughout the study, indicating that CKRT did not significantly or independently cause thrombocytopenia [45]. There was no significant association between changes in platelet counts and 90-day mortality when employing multivariable Cox regression analysis (HR = 0.79, 95% CI = 0.18–3.50, P = 0.76). However, when analyzing the change in platelet count based on non-reduction versus reduction among survivors, a decrease in platelet count was associated with higher mortality at 90 days (HR = 1.54, 95% CI = 1.08–2.20, P = 0.02).
Bai and colleagues conducted a meta-analysis of 11 RCTs with 992 patients and 1,998 circuits, which revealed no significant differences in patient survival between citrate and heparin anticoagulation [138].
3.11.2. Bleeding Risk
In a meta-analysis of 11 RCTs with 992 patients and 1,998 circuits, Bai and colleagues evaluated the safety and efficacy of citrate versus heparin anticoagulation for CKRT in critically ill patients [138]. They reported that the incidence of HIT and the risk of bleeding were lower in the citrate group (RRs: 0.46 and 0.34, respectively) compared to the heparin group. This finding aligns with another meta-analysis conducted by Wu et al. [125]. Additionally, Morabito et al. suggest that a no-anticoagulation approach could ensure adequate filter life in patients at risk of bleeding and/or thrombocytopenia [139].
A single-center retrospective analysis involving 71 adults with acute liver failure or decompensated cirrhosis evaluated the effects of CKRT without anticoagulation or with heparinization in an intensive care unit (539 circuits) [140]. Among the 71 patients, 33 experienced significant bleeding events. Using multivariate logistic regression, researchers found that patients with higher baseline Activated Partial Thromboplastin Time (APTT), those receiving vasoactive drugs for over 24 hours, or those with thrombocytopenia had a higher incidence of bleeding complications (P < 0.05) [140].
3.11.3. Infection Risk
Griffin et al. retrospectively evaluated a cohort of 747 ICU patients, among whom 253 had thrombocytopenia at the initiation of CVVH [23]. They reported that patients with over a 40% decrease in platelet counts who survived to discharge faced a 49% increased risk of post-ICU infections. The risk of post-ICU shock was also elevated, though not significantly. The authors concluded that if platelet counts at the start of CKRT were below 100 x 103/μL, and there was a drop of more than 40% during treatment, the risk of post-ICU infections nearly doubled, especially in patients who already had thrombocytopenia at the outset of CKRT [23].
3.11.4. Kidney Recovery
Griffin et al. also evaluated the extent of relative and absolute reductions in platelet counts related to kidney recovery in their secondary analysis of RENAL trial data [136]. They discovered that nadir platelet values below 100,000/µL and a decrease in platelet count greater than 50% after the initiation of CKRT were linked to lower kidney recovery rates (independently of KRT) and fewer KRT-free days [116]. Furthermore, they found that baseline thrombocytopenia before starting CKRT was associated with diminished recovery of kidney function [136].
3.11.5. Filter/circuit Life
A Spanish study in 61 AKI patients assessed filter life in patients undergoing CKRT. In total, 122 filters were utilized [141]. Patients were categorized based on Anticoagulation (AC) with UFH versus no Anticoagulation (No AC). The investigators did not identify any statistically significant differences in filter lifespan between the two groups (30.5 hours AC vs. 34.9 hours No AC). However, the mean platelet counts in both groups decreased from baseline to post-CKRT (AC: 131.3 to 118.8 x 109/L; No AC: 78.2 to 68.1 x 109/L). Notably, patients with severe thrombocytopenia at baseline were placed in the No AC group. In contrast, mild thrombocytopenia was noted in the AC group at baseline, highlighting the various factors involved in developing thrombocytopenia.
Fifty-nine patients underwent CKRT for Acute Kidney Failure (AKF) following cardiac surgery. Patients who met one of the following criteria were chosen for no-anticoagulation CKRT: spontaneous bleeding, Activated Partial Thromboplastin Time (APTT) >45 seconds, thrombocytopenia, and recent surgery (< 48 hours) [139]. A filter life of less than 24 hours without anticoagulation was the threshold for initiating regional anticoagulation CKRT. Heparin was infused pre-filter and protamine post-filter at an initial ratio of 1 mg protamine to 100 IU heparin for regional anticoagulation. This ratio was adjusted to achieve a patient APTT of less than 45 seconds and a circuit APTT greater than 55 seconds. Twenty-two patients (37.3%) were selected for no anticoagulation. Twelve patients continued with no anticoagulation (filter life: 38.3 ± 30.5 hours), while 10 transitioned to regional anticoagulation (filter life: 38.6 ± 25 hours). During regional anticoagulation, no significant difference was found between baseline APTT (36.7 ± 6.4 seconds) and patient APTT (41.5 ± 12.6 seconds), while circuit APTT (77.7 ± 43.3 seconds) was significantly higher than patient APTT (P < 0.0001). The probabilities of the circuits remaining free from clotting after 24, 48, and 72 hours were: a) no anticoagulation: 55.5%, 30.1%, and 16.6%, and b) regional anticoagulation: 76.2%, 39.6%, and 19.8%. No systemic anticoagulation was observed after regional anticoagulation CKRT was terminated.
Chua et al. reported a median overall lifespan of the circuit of 9 (6-16) hours, with a 12-hour (7-24) average in 51 patients who were not anticoagulated [140]. In the 20 patients who received heparinization, the circuit life was not significantly different at 7 (5-11) hours despite the increased heparin dosage. Using multivariate linear regression, patients with higher baseline APTT, serum bilirubin, or those not mechanically ventilated had longer circuit lifespans (P < 0.05). Decreasing platelet counts (especially <50 × 109/μL) had small but significant effects on circuit lifespan (P < 0.0001).
Another meta-analysis of 16 randomized controlled trials involving 1,229 patients found that the circuit lifespan in the regional citrate group was 15.37 hours longer (95% CI, 10.09-20.65, P < 0.00001) than in the heparin group (excluded due to Chinese language) [142]. The authors recommend using RCA over heparin to prolong the circuit lifespan and reduce the risk of bleeding in critically ill patients. A systematic review and meta-analysis of six RCTs with 488 patients showed no significant difference in circuit survival time or thrombocytopenia between the RCA and heparin groups [143]. However, a notable degree of heterogeneity was observed among the included studies.
A retrospective analysis of CKRT circuit life in 50 patients with acute liver failure, Acute On Chronic Liver Disease (ACLD), or post-elective Liver Transplantation (LTx) was conducted, featuring two control groups: Systemic Sepsis (SS) and Hematological Malignancy (Hem) [144]. Patients with hematological malignancies had significantly lower platelet counts than the sepsis group (P = 0.0045) but did not differ from the liver groups. By utilizing a multiple logistic regression model, the authors identified that initial CKRT circuit life and the number of CKRT circuits used within the first 48 hours were influenced by initial peripheral platelet count, prothrombin time, activated partial thromboplastin time, the vascular access site, the use of lactate-based replacement fluids, the rate of fluid exchange, the use of anticoagulants, transmembrane pressure, and patient demographics. They concluded that their data did not show any associations between laboratory clotting times, peripheral platelet count, and the duration of the first CKRT circuit. Additionally, the survival advantage of the CKRT circuit was not associated with decreased platelet count, increased laboratory prothrombin ratio, or clotting times.
Intermittent hirudin is safe for anticoagulation in CKRT; however, better filter survival has been reported with heparin, although heparin can induce HIT [145]. Direct thrombin inhibitors, such as argatroban, are also viable options for anticoagulation in CKRT, particularly for patients with HIT [102]. In cases where argatroban is contraindicated, such as in liver failure patients with HIT, recombinant hirudin (lepirudin) may be used [146]. Tsu and colleagues retrospectively assessed 135 patients treated with bivalirudin for HIT from 2004 to 2009 [105]. The patients were classified based on kidney function, with those receiving dialysis further divided into three subgroups according to the mode of hemodialysis: IHD (n = 24), sustained low-efficiency daily diafiltration (SLEDD, n = 12), or CKRT (n = 5). Of the 135 patients, 100 experienced thrombocytopenia, with the platelet nadir in CKRT patients averaging 52.2 (42.5) x 103/μL. Anticoagulation doses required to achieve APPT target values were significantly higher for patients on SLEDD than those on IHD or CKRT (45% lower), suggesting a need for dosing adjustments.
3.11.6. ICU Length of Stay
A retrospective cohort study involved all patients at a general ICU receiving CKRT for 14 months [147]. Patients were stratified according to anticoagulant use, specifically prefilter prostaglandins (n = 24) or prefilter heparin (n = 70). The ICU stays were divided into three periods: before, during, and after CKRT. The prostaglandin group was more severely ill, exhibiting lower platelet counts at the onset of CVVHDF. During CKRT, this group experienced a higher incidence of Disseminated Intravascular Coagulation (DIC) (58% vs. 26%; P = 0.006) and severe thrombocytopenia (71% vs. 44%; P = 0.03), along with elevated maximum Sequential Organ Failure Assessment scores (P <0.001) and a greater frequency of blood transfusions (P = 0.006) in comparison to the heparin group.
3.12. Management and Prevention
Although no clear guideline recommendations explicitly address the prevention and management of CKRT-associated thrombocytopenia, some approaches to managing or mitigating this complication have been discussed in the medical literature [125]. Precautionary measures to reduce platelet loss in critically ill patients undergoing CKRT, as reported in a single-center study by Wu et al., might include the preferential use of cellulose-based, non-e-beam-sterilized hemofilters, preserving circuit patency, employing regional citrate anticoagulation in patients at risk for bleeding, combining anticoagulation with tirofiban (a platelet aggregation inhibitor) and unfractionated heparin, using low molecular weight heparins or prostacyclin instead of unfractionated heparin, and administering argatroban instead of unfractionated heparin in patients with heparin-induced thrombocytopenia [125]. Additionally, a small pilot study found that the use of an antiplatelet IIb/IIIa receptor inhibitor could mitigate platelet loss and help maintain platelet function in patients receiving CKRT; however, the use of antiplatelet agents to enhance outcomes has not been adequately substantiated [23, 102].
Since the etiology and significance of CKRT-associated thrombocytopenia are poorly understood, its emergence frequently leads to a thorough investigation for conditions such as Heparin-Induced Thrombocytopenia (HIT) and other potential underlying comorbidities. Patients receiving heparin for anticoagulation may be at risk for HIT, and while HIT accounts for only a tiny percentage of thrombocytopenia cases in critically ill patients, up to 25% of CKRT patients who experience early filter clotting may test positive for HIT antibodies [148]. Finkel et al. suggest that HIT is more likely to occur when the degree of thrombocytopenia is moderate, with heparin exposure lasting 5-10 days and signs of thrombosis present [148]. When HIT is suspected, heparin must be discontinued until diagnostic test results are available, followed by the initiation of an alternative anticoagulant [10, 47, 148].
Although the 2012 American College of Chest Physicians HIT guidelines did not provide specific guidance for patients on ECLS, they did recommend bivalirudin for patients with acute HIT who require urgent cardiac surgery compared to other agents. They also suggested bivalirudin or argatroban for patients with HIT who need percutaneous coronary interventions. In a systematic review and meta-analysis involving 28 ECLS patients, 22 patients (78.6%) were treated with argatroban, 4 (14.3%) with bivalirudin, and 2 (7.1%) with lepirudin [149].
Some studies have also reported on the use of alternative anticoagulants, saline flushes, or thromboprophylaxis to manage and prevent thrombocytopenia in CKRT [47, 54, 141]. As mentioned earlier, proper monitoring for the onset of thrombocytopenia is a crucial aspect of patient management [124].
4. DISCUSSION
In this study, we aimed to understand the totality of the data related to the impact of thrombocytopenia in CKRT. This is the first systematic review that assesses whether thrombocytopenia during CKRT is clinically relevant. Our review revealed 85 studies with 29,217 patient samples that we included in our analysis. Consensus indicates that thrombocytopenia is a common and highly variable issue in critically ill patients, with several studies reporting an increase in its occurrence following the initiation of CKRT. The severity of thrombocytopenia is also quite variable. Multiple factors contribute to thrombocytopenia during CKRT, including membrane types, sterilization techniques, devices, therapies, flow rates, medications, and underlying conditions. These were identified in RCTs, systematic reviews and meta-analyses, NRSIs, reviews and guidelines, and case studies. However, the quality assessments found that for the RCTs, the overall risk of bias was high or unclear across all the studies, suggesting low quality. The overall quality of the cohort studies was poor, and no high-quality systematic reviews or meta-analyses were identified. In addition, the overall evidence related to thrombocytopenia epidemiology, severity, proposed causative mechanisms such as membrane effects, sterilization techniques, flow rates, and clinical outcomes like infection risk, kidney recovery, and ICU length of stay during CKRT was of low certainty. Data on thrombocytopenia occurrence due to devices used, medications, and underlying conditions were of moderate certainty, and clinical outcomes of mortality or survival, bleeding risk, and filter or circuit life were of high certainty. Generally, data addressing the management and prevention of CKRT-induced thrombocytopenia were of high certainty, with a low risk of bias. Therefore, the publications identified could be used to assess the clinical relevance of thrombocytopenia during CKRT.
To understand the variation and effect sizes of the populations in the different categories of studies, we calculated means, standard deviations, the pooled standard deviation, and Hedges’ g values. For all categories except case studies, the standard deviations were larger than the means, suggesting high variability within the identified studies. Hedge's g is an effect size statistic that measures the standardized difference between two group means and incorporates a correction factor to reduce bias. Effect sizes are generally rated as small (<0.2), medium (0.2-0.7), or large (≥0.8) [21]. The smallest effect sizes were observed between RCTs and cohorts (retrospective: 0.22, prospective: 0.26, Table 2). This suggests that the information obtained from these three groups was similar. Moderate “g” values were calculated when RCTs and prospective cohorts were compared to case studies (0.66 and 0.47, respectively), suggesting moderate differences between these groups and case studies. Large effect sizes from Systematic Reviews/Meta-analyses indicate that data from systematic reviews show a more substantial effect on the outcome of CKRT-derived thrombocytopenia. In contrast, data from RCTs showed weaker-than-expected effect sizes. This was somewhat surprising, but it may be due to the considerable variation from the mean across all studies. Retrospective studies had a larger effect size than prospective studies or case studies, suggesting that these are large enough to determine effects. Therefore, the sample size (29,217) is large enough to evaluate epidemiology, proposed mechanisms, possible outcomes, management, and prevention of thrombocytopenia during CKRT.
Out of the 119 papers included for assessment, 85 were relevant for assessing the impact of thrombocytopenia during CKRT; the remainder consisted of expert reviews and guideline recommendations and were not used for calculating patient numbers or effects. Hedges’ g values in Table 4 provide insight into the effect sizes for 19 parameters. Overall, the assessment showed very small effect sizes for the large categories of epidemiology, clinical outcomes, and management and prevention, suggesting that potential conclusions from these areas may be weak. Small to moderate effect sizes for severity and proposed mechanisms of thrombocytopenia. Delving deeper into the proposed mechanisms, we identified that the effects are probably driven by publications related to device use, membrane type, and sterilization methods. When analyzing the various clinical outcomes, we found moderate to large effect sizes for all categories except reversibility (g =0.18, small). Together, these suggest that underlying conditions may heavily impact outcomes.
Despite the small “g”, data identified that CKRT-associated thrombocytopenia may be reversible or can rebound following the cessation of therapy. This was reported by Droege et al., Ferreira et al., Kontny et al., and Gionis et al. [10, 24, 129, 130]. Changing the parameters during CKRT, such as the blood flow rates, dialyzer type, or sterilization, was also shown to promote platelet rebounds [36, 40, 41, 62]. Various therapeutics may also increase the risk of thrombocytopenia, which may be reversible following discontinuation of use [83, 107, 115, 122, 123]. Using RCA instead of heparin in patients with suspected or confirmed HIT also prevented significant platelet drops [41, 42, 47, 68]. Lin et al. reported that CKRT did not significantly or independently cause thrombocytopenia and was not associated with increased 90-day mortality [45]. Bai et al. also pointed out that the use of citrate or heparin as the anticoagulant did not have any relevant impact on survival [138]. In addition, kidney recovery was impacted by baseline platelet levels [136]. Together, these studies indicate that underlying conditions likely affect outcomes more than CKRT itself. Therefore, timely treatment of underlying comorbid conditions that contribute to thrombocytopenia could help prevent platelet decline [5, 10, 124, 132] and facilitate better platelet recovery.
Though it is difficult to determine what patients could tolerate as the absolute nadir, Goff et al. [35] reported the lowest platelet count of 13 × 109/L that rebounded slowly after cessation of CKRT. However, details of the study were not published as a peer-reviewed manuscript. Drug therapies have led to platelet levels 15-20 × 109/L, with rebound effects seen after discontinuation. It may also be prudent to prevent platelet drops greater than 50% of baseline during any given treatment, as this may lead to slow or ineffective recovery.
Despite the poor quality of published and available data, various etiologies and comorbidities appear to facilitate and sustain the development of thrombocytopenia in critically ill patients undergoing CKRT, making it unlikely that a single study will identify one specific cause under the prevailing circumstances. Consequently, the precise mechanism behind the emergence of thrombocytopenia in individuals undergoing CKRT is multifactorial, with numerous potential explanations proposed, including uremia, sepsis, disease severity, mechanical support, the CKRT circuit itself, and the use of heparin or other medications. Additionally, research has identified several risk factors for thrombocytopenia in patients receiving CKRT, with low SOFA scores, low platelet counts at CKRT initiation, and existing comorbid conditions consistently associated with an increased risk. In patients affected by one or more of these factors, thrombocytopenia can impede the recovery of kidney function and heighten risks of infection and mortality.
Variability in reported etiologies and risk factors likely arises from the diverse and inconsistent disease definitions used and the comorbidities present in critically ill patients requiring CKRT. Insufficient patient sample sizes, heterogeneity in patient populations, and multiple limitations in study design also contribute to the poor quality of data identified and the inability to determine causality or the effectiveness of treatments. To mitigate potential shortcomings and risks, regularly monitoring patients receiving CKRT for known contributors to thrombocytopenia could improve the timing of identification and enable early and appropriate management.
To the authors’ knowledge, this is the most comprehensive assessment performed on this topic. The chosen articles met the inclusion criteria and were analyzed using multiple tools appropriate for each study design. The certainty of the evidence was also determined. Each included study was reviewed by three independent reviewers, with adjudication when needed. A large, highly relevant patient population was included in multiple study designs, allowing for coverage by real-world data and controlled studies. The systematic approach with a broad search string and without time boundaries across three primary databases minimizes the risk of overlooking relevant studies. This lends internal validity and increases generalizability to different populations of critically ill patients requiring CKRT. Despite the comprehensive nature of this analysis, there are several limitations. First, the authors did not perform a meta-analysis to determine numerical levels of influence by the individual factors because much of the raw data was missing. Second, the data identified and included in the analysis were generally of low quality with a high risk of bias. This could adversely impact the overall interpretation of the results. Hedges’ g was used to determine effect sizes at a high level, which may not have appropriately determined the effect size of the individual study. This could adversely impact the overall interpretation of the results. Third, thrombocytopenia definitions differ considerably across various studies, making accurate determinations difficult. Fourth, several studies were included as pertinent data for CKRT protocols. However, they were not included in the analysis because they did not directly address thrombocytopenia. In addition, the data from drug studies, as opposed to those in devices, were of better quality and certainty. Finally, whether CKRT-induced thrombocytopenia is clinically relevant may be subjective based on the physician’s experience. Thus, reporting biases may have been unknown in some studies.
CONCLUSION
To our knowledge, this is the first comprehensive assessment of thrombocytopenia in CKRT patients. It is the first to conclude that CKRT-induced thrombocytopenia appears reversible and may not be clinically significant unless affected by additional risk factors, including medications and existing comorbid conditions. Based on our evaluation of the available information, the impact of CKRT on thrombocytopenia depends on the patient’s status and treatment goals. If the patient’s recovery potential is good and imminent, and thrombocytopenia is not severe or influenced by low-risk factors, the activation of thrombocytopenia due to CKRT may not be clinically relevant. This systematic review gives healthcare practitioners a better and more thorough understanding of thrombocytopenia during CKRT.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: D.T.: Study conception and design; N.W., T.T.: Data collection; D.A.S.: Study design, conceptualization, and writing. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| DIC | = Disseminated Intravascular Coagulation |
| SLE | = Systemic Lupus Erythematosus |
| CKRT | = Continuous Kidney Replacement Therapy |
| CRRT | = Continuous Renal Replacement Therapy |
| CVVH | = Continuous Venovenous Hemofiltration |
| CVVHD | = Continuous Venovenous Hemodialysis |
| CVVHDF | = Continuous Venovenous Hemodiafiltration |
| HT | = Heparin-Induced Thrombocytopenia |
| PIKRT | = Prolonged Intermittent Kidney Replacement Therapy |
| CPB | = Cardiopulmonary Bypass |
| ECMO | = Extracorporeal Membrane Oxygenation |
AVAILABILITY OF DATA AND MATERIALS
All the data and supporting information are provided within the article.
CONFLICT OF INTEREST
Dr. Dixie-Ann Sawin is on the Editorial Advisory Board of The Open Urology & Nephrology Journal.
ACKNOWLEDGEMENTS
Declared none.

