All published articles of this journal are available on ScienceDirect.

LEARNING FROM IMAGES Size Matters
Arteriovenous fistula (AVF) is considered the preferred vascular access to provide maintenance hemodialysis for its known lower incidence of morbidity and mortality compared to arteriovenous graft and central venous catheters. Nevertheless, early maturation failure and development of stenosis remain major hurdles leading to AVF dysfunction. Endovascular stent placement is often necessary to treat stenosis that recurs frequently or demonstrates significant elastic recoil despite adequate angioplasty. The decision to place an endovascular stent is complex and involves selecting a suitable candidate and choosing an appropriate stent. The length and luminal diameter of the stent need to be selected very carefully for treating venous stenosis. Unlike arteries, the veins are thin walled, compliant and tend to dilate easily. In the case of central veins, the venous diameter can differ with the variations in intrathoracic pressure related to respiration.
In the case presented in this report, a recurrent outflow stenosis in an upper arm brachiocephalic AVF was treated with two overlapping, inadequately sized bare-metal stents (Fig. 1). A high blood flow in an upper arm AVF combined with non-compliant stented segment of the outflow vein resulted in the development of aneurysmal dilatation distal to the stent. Stent deployment in an AVF and arteriovenous graft (AVG) should preferably be reserved for endovascular emergencies such as vascular tears and in high-risk surgical candidates [1]. Surgical revision is a preferred option whenever possible. Stent deployment should be clearly avoided in the cannulation segment of the AVF [2]. Accidental cannulation of the stent for dialysis can increase the risk of stent rupture with protrusion of the sharp end through the skin and can be a potential hazard to the dialysis staff [3].
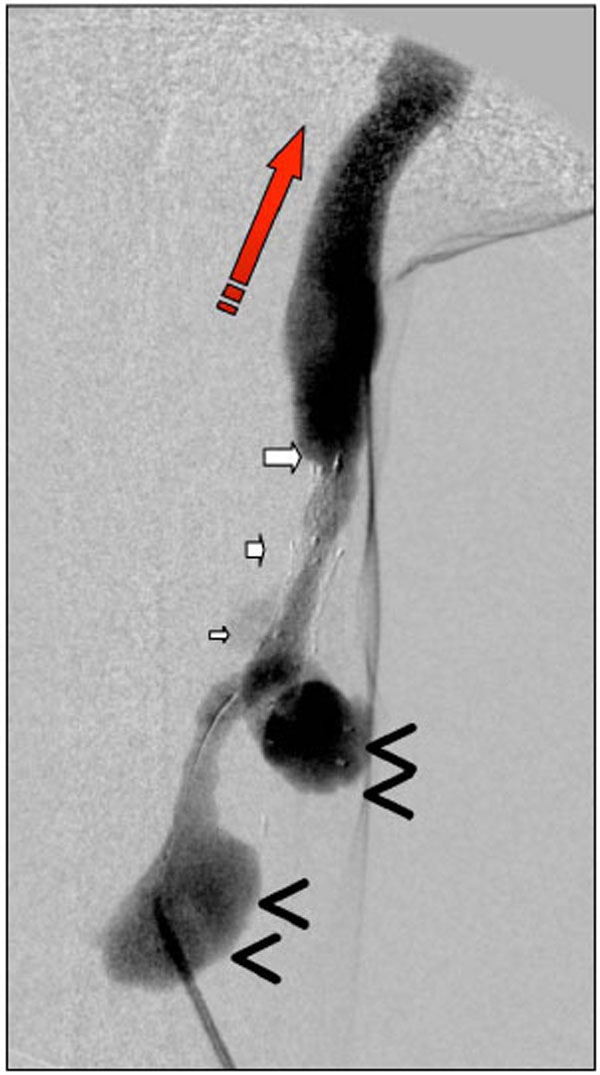
An upper arm arteriovenous fistula with inadequately sized bare-metal stents in the outflow segment (marked by white arrows) leading to aneurysm (marked by black arrow-heads) formation in the distal segment. The direction of the blood flow is indicated by the red arrow.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

