All published articles of this journal are available on ScienceDirect.

Correlation of Sacral Ratio and Urinary Tract Infection in Children
Authors Info & Affiliations
Abstract
Introduction:
The sacral bone anomalies have an important effect on urinary and gastrointestinal tract and sacral ratio was defined as an indicator for estimating the anorectal abnormalities in children. This study was carried out for determining the association between sacral ratio and Urinary Tract Infections (UTI) among children.
Material and Methods:
In a cross sectional study, 100 children under 15 years with proven febrile UTI were referred to a referral children center considering the presence and grading of VUR according to VCUG enrolled in this study.
Sacral ratio was measured for all cases and the data were compared by student T test, Chi 2 and Mann Whitney tests. SPSS 16.0 software was used for data analysis. P values less than 0.05 were considered significant.
Results:
41 boys and 59 girls with mean age 4.8 years were enrolled in this study. The average range of sacral ratio was 0.82. There was no staistical difference between two different genders and ages (p > 0.05).
The values of SR in patients with VUR were lower than patients without VUR(P˂0.05) but there was no statistically significant difference between both bilateral and unilateral VUR and SR (p > 0.05).
Conclusion:
The risk of sacral bone abnormality in patients with VUR is more than patients without VUR. Therefore, in patients with UTI and low SR simultaneously, tighter evaluation for VUR and treatment should be considered.
1. INTRODUCTION
Urinary Tract Infections (UTI) are considered as the most common bacterial infections among children. The prevalence of UTI is estimated 2% in boys and 8% in girls [1, 2]. UTI can predispose the patients to increase the risk of renal failure due to renal scarring and hypertension and end stage renal disease in pediatric population. Sacral bone abnormality like hypoplasia or agenesis is one of the important risk factors for urinary dysfunction [2]. Recurrent UTI is defined as a further infection by a new organism. Relapsing UTI is defined as a further infection with the same organism. The recurrent infections can result in renal scarring, which can lead to renal hypertension and end-stage renal disease [3]. Although using new diagnostic tests and appropriate treatment, the mortality and morbidity of UTI are diminished significantly, but UTI is an important factor producing structural dysfunction, progressive renal failure, hypertension and also renal stones [2]. Although the complication does not occur in most patients after treatment, but also identifying the susceptible patients is very important for the prevention of complication [3, 4]. Acute pyelonephritis and VUR are diagnosed as two synergistic factors producing the destruction in pediatric kidneys [4]. Vesicoureteral Reflux (VUR) is an important urological abnormality which can cause recurrent febrile UTI in childhood. Obstructive anomalies are found in up to 4%, and VUR in 8% to 40% of children being investigated for their first UTI. The recurrent UTI can be complicated by renal scarring, which can lead to renal hypertension and end-stage renal disease [5]. Many authors consider the Long-term antibiotics for preventing recurrent urinary tract infection in pediatric population [6, 7]. In some investigations antibiotics of choice for preventing gram negative microorganisms are suggested by authors [8, 9], although Ian et al. showed early treatment of acute pyelonephritis in children fails to reduce renal scarring [10]. In purpose to detect urinary tract anomalies, VCUG (voiding cystourethrogram) is the most useful methods in children ([11, 12] The potential role for MRU (Magnetic Resonance Urogram) in the diagnostic work-up of upper urinary tract dilatation in infants and children is showed by some authors [13, 14]. Diagnostic strategies of interstitial cystitis due to infections were described by Patnaik [15]. Sacral bone abnormality like hypoplasia or agenesis is one of the important risk factors for urinary dysfunction [2].
The relationship between sacral agenesis and VUR, enuresis, voiding dysfunction, and neurogenic bladder is well known previously [16-20].
Pena et al. suggested the Sacral Ratio (SR) for evaluation of sacral development. Sacral ratio was calculated according to Pena criteria in plain lumbosacral spinal radiography [16]. Three lines were drawn for each pelvic radiograph, a line is drawn connecting the upper zone of both iliac crests, the second line was connecting the most inferior point of the sacroiliac joints and the third line parallel to other lines across the inferior points of the sacrum. By dividing the distance between the two baseline (on the distance between the two upper lines sacral ratio were calculated [16]. MC Lellan et al. reported the relationship between sacral anomalies and urinary dysfunction [17]. Sacral index is a marker which were used for identifying the predisposing risk factors for UTI, urinary dysfunction, VUR, constipation and also urinary incontinence [17]. Correlation between SR and anorectal anomalies were evaluated by Macedo et al. and others [18-20].
UTI is a common cause for hospital admission among Iranian children [21-24]. A prospective clinical study by some Iranian workers determined the incidence of renal scarring following acute pyelonephritis and previously well-known risk factors such as VUR, age and recurrent urinary tract infections [21]. Association of voiding dysfunction following sacral anomalies was considered in the previous Iranian studies [24, 25].
The aim of present study was determination of average SR among children with UTI admitted in pediatric ward of Rasul Akram Hospital during 2008-2016.
2. MATERIALS & METHODS
This cross sectional study were performed upon 100 children (< 15 years old) with proven febrile UTI who were admitted in pediatric department in Rasoul Akram Hospital, Tehran, Iran during 2008-2016.
The patients with structural sacrum anomaly included myelomeningocele and sacrococcygeal teratoma, imperforated anus, lipomeningocele and all children with history of trauma or pelvic fracture were excluded from the study.
Diagnostic criteria: UTI was diagnosed as positive urine culture with more than 105 colony-forming units per milliliter of a single pathogen or 104 colonies in a symptomatic patients or > 50000 colonies of a single pathogen in obtained samples via suprapubic or catheter [1].
VCUG was performed for all cases within 6 weeks after urinary tract infection. Sacral ratios were calculated according to Pena criteria in plain lumbosacral spinal radiography [16]. Three lines were drawn for each pelvic radiograph, a line is drawn connecting the upper zone of both iliac crests, the second line was connecting the most inferior point of the sacroiliac joints and the third line parallel to other lines across the inferior points of the sacrum. By dividing the distance between the two baseline (BC) on the distance between the two upper lines (AB), sacral ratio was calculated. The normal limits of SR were considered as >/= 0.74 in anteroposterior and >/= 0.77 in lateral view according to Pena et al. criteria [16].
All data were entered in the check list and finally were analyzed by SPSS 16.0 software.
3. RESULTS
One hundred children (mean age 4.8 years and SD of 3.2 years) were enrolled in the study. 41 (41%) of the total cases were male and 59 (59%) were female.
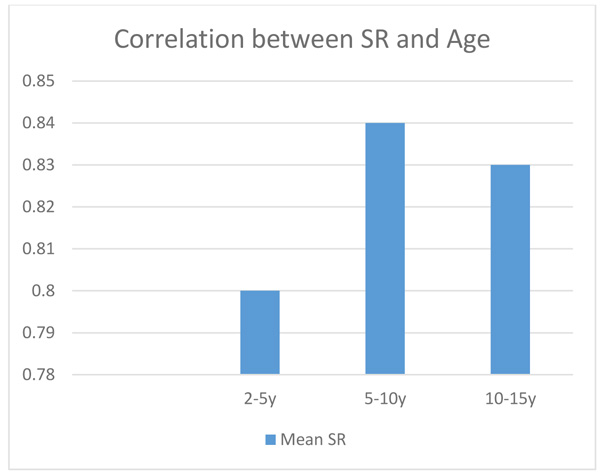
The patients were divided to 3 groups according to age. The average SR in patients between 2-5 years was 0.80 with 0.079 SD and for cases between 5-10 years and 10-15 years was 0.84 (SD : 0.076) and 0.83 (SD : 0.07) respectively (Fig. 1). The average SR in girls was 0.81 with 0.076 SD and in boys was 0.85 with 0.08 SD. There was no significant difference between SR and age and gender (p > 0.05).
The cases were divided into four groups according to the existence of VUR and also VUR grading. The SR scales in relation to VUR and grading were compared which are shown in Table 1.
| VUR | Mean | Minimum | Maximum |
|---|---|---|---|
| Grade 1 | 0.85 | 0.63 | 0.90 |
| Grade 2 | 0.82 | 0.64 | 0.92 |
| Grade 3 | 0.80 | 0.70 | 0.95 |
| Without VUR | 0.87 | 0.62 | 0.94 |
There was no significant difference among the patients with unilateral VUR and SR (average = 0.81 and SD 0.076) and also the patients with bilateral VUR and SR (average = 0.84 with SD 0.71 (P > 0.05). But SRI decreases in parallel to increasing VUR grading. This index in patients without VUR has higher mean level in comparison to children with VUR.
4. DISCUSSION
In the present study we investigated the relation between SRI and VUR in children (< 15 years old) with proven UTI. According to our results no significant difference was observed between age and gender with SRI. No correlation between unilateral VUR and SRI (average = 0.81 and SD 0.076) and bilateral VUR and SR (average = 0.84 with SD 0.071) had found in our studied cases. SRI decreases in parallel to increasing VUR grading. This index in patients without VUR has higher mean level in comparison to children with VUR.
SRI (Sacral index) was a marker which were used for identifying the predisposing risk factors for UTI, urinary dysfunction, VUR, constipation and also urinary incontinence [16-18] and low SR index which represent the sacral bone development can in turn create urinary system disorders [16].
Kajbafzadeh et al. investigated the correlation of SR index and results of VUR among 30 children with UTI and controls. They found no significant difference between age and this index, compatible to our results [19]. Yousefichaijan et al. reported the sacral Index in children suffering from different grades of VUR [20].
According to the results of the present study, in parallel to increasing the VUR grading, the sacral index is diminished, but because existence of sacral bone anomalies was not considered, SR was used as an independent factor in relation to VUR and considering the chance of simultaneous occurrence of abnormal SR and VUR, in the absence of sacral anomaly due to close embryonic origin of sacral bone and bladder or neurogenic infrastructural abnormality in patients with abnormal SR and also insufficient sample size, other studies with higher sample size are needed. On the other hand, abnormal SR can be recognized as a risk factor for predicting UTI occurrence, therefore these cases can be evaluated for UTI occurrence from earlier ages.
CONCLUSION
The risk of sacral bone abnormality in patients with VUR is more than patients without VUR. According to the results of present study, SR decreases in parallel to increasing VUR grading. This index in patients without VUR has higher mean level in comparison to children with VUR.
Therefore, in patients with UTI and low SR simultaneously, tighter evaluation for VUR and treatment should be considered.
Considering relationship between SR and occurrence of VUR, correlation of this index with UTI, point of determination and also prediction of prognosis, the treatment programs can be planned meticulously.
LIMITATION OF THE STUDY
Our study included a relatively small sample size and lacked of long-term follow up.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical Committee in the Pediatric Infectiuos Diseases (affiliates by Iran University of Medical Sciences) has reviewed and approved the Waiver of Authorization for use of protected health information (PHI) for research purposes for the following study and the number is 92-01-131-25731.
HUMAN AND ANIMAL RIGHTS
Animals did not participate in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2008.
CONSENT FOR PUBLICATION
Consent for publication was obtained.
CONFLICTS OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
The research team wish to thank vice chancellor of research for their financial support and also children and their parents who contribute to this research.

