All published articles of this journal are available on ScienceDirect.

A Rare Case of Co-occurrence of Emphysematous Cystitis and Emphysematous Myositis in a Haemodialysis Patient
Abstract
Urosepsis presents an unusual diagnostic challenge in chronic dialysis patients who often are anuric. This leads to atypical presentations, delayed diagnosis and poor outcome. Here we present a case of an elderly diabetic patient with chronic kidney disease on maintenance haemodialysis who presented with lower limb pain initially and had no urinary complaints. The evaluation revealed the presence of extensive emphysematous pyelonephritis, cystitis and myositis. The unusual presentation is discussed along with a relevant review of the literature.
1. INTRODUCTION
The diagnosis of urinary tract infection and urosepsis is difficult in dialysis patients. The uraemic state precludes the mounting of a febrile response, which is particularly true in the elderly and diabetic patients.The chronic dialysis patients are often anuric with the result that the patients do not complain about urinary urgency, frequency or dysuria being the typical features in the normal population. [1] Here we present one such elderly dialysis patient who had atypical presentation with the result that urinary infection was diagnosed late, resulting in fatality.
2. CASE REPORT
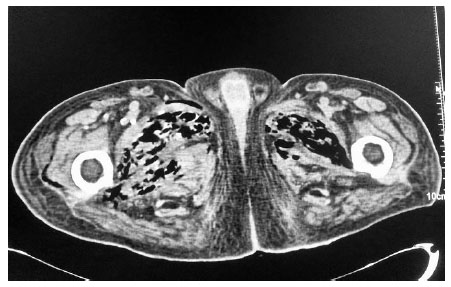
An elderly gentleman, aged 83 years, with diabetic end-stage renal disease, who was on maintenance haemodialysis, complained of severe pain in both the thighs when he came for his scheduled dialysis. He reported that the pain was severe, and he was unable to walk and attend his activities of daily living (ADL). He presented no history of fall or fever. He had been receiving twice weekly haemodialysis through left brachiocephalic arteriovenous fistula for the last one year. His regular medications included human premixed insulin 8 units daily, sustained release of Nifedipine 20 mg twice daily along with tab calcium carbonate and vitamin supplements.He was ambulatory and required no assistance for ADL earlier. His diabetic status and blood pressure were fairly under control till this event. Examination revealed no inflammatory signs. There was no evidence of fracture clinically and he was prescribed some anti-inflammatory drugs. He returned for his scheduled dialysis again after three days complaining of persistent pain. He appeared sick, but was stable hemodynamically. He was in severe agony with his slightest movement.There was local tenderness but no other inflammatory signs. He could complete haemodialysis without event and refused further investigations. He returned for the scheduled dialysis again after three days. This time, he reported fever with chills for two days prior to the hospital visit and presented in a moribund state. He was febrile and had excruciating pain in both the thighs. The slightest movement of lower limbs caused him severe pain. His vitals included BP of 180/110 mm of Hg, pulse rate of 130 beats/min and respiratory rate of 24 cycles per minute. He was conscious and fully oriented. He had severe tenderness in the lower abdomen and in both the thighs with no other inflammatory signs.Laboratory investigations revealed haemoglobin 11.1gm/dl, total leucocyte count 24300 cells/cu mm with polymorphonuclear neutrophil predominance and a platelet count of 213000 cells /cu mm. Random blood sugar was 501 mg/dl. Serum creatinine, calcium and phosphorus were 6.4, 9.8 and 5 mg/dl, respectively. He had normal serum electrolyte and uric acid. ABG revealed metabolic acidosis with a pH of 7.21 and serum bicarbonate being 11.2 mmol/l. Liver function test was normal except serum albumin of 3.0 g/dl. Urine was negative for ketones but microscopic examination showed 20-25 pus cells and red blood cells. Urine and blood culture both grew Escherichia coli. His chest X ray was normal. Ultrasound examination of the abdomen showed the presence of gas in the bladder and due to disproportionate symptoms, non-contrast CT scan abdomen was ordered. The CT scan revealed extensive mottled air pockets in the muscles of bilateral upper thigh, predominantly involving adductor compartments, right more than left Fig. (1). There was thickening of the urinary bladder wall with perivesical fat stranding and intramural as well as intraluminal air consistent with emphysematous cystitis Fig. (2). Mild left emphysematous pyelonephritis was also noted Fig. (3). He was treated with IV meropenem and Levofloxacin. Foley’s catheter was inserted for bladder drainage. Insulin infusion was started. However, he weakened quickly, became hypotensive and disoriented. Following this, haemodialysis was intensified, so he was treated with inotropic infusions and other supportive measures.The patient’s family refused surgical options.He succumbed 4 days after admission.


3. DISCUSSION
Emphysematous urinary tract infections are necrotizing infections of the urinary tract associated with the presence of gas in the renal parenchyma, pelvis or perinephric space. [2] Escherichia coli and Klebsiella pneumoniae are the most common pathogens. Rarely, other pathogens like Enterobacter aerogenes, Proteus mirabilis, Staphylococcus aureus, Streptococci, Clostridium perfringens, Nocardia and Candida albicans may also contribute.[3] Diabetes mellitus and urinary tract obstruction are important predisposing factors.[2] These infections are rapidly progressive and they carry significant morbidity and mortality unless rapidly diagnosed and aggressively treated. Diagnosis depends on the demonstration of gas within the urinary tract. Although in extensive EPN, gas in the renal system can be demonstrated on Plain X-ray KUB, and CT scan KUB appears to be the diagnostic modality of choice.The pathogenesis of emphysematous infection of the urinary tract is said to be due to the rapid destruction of the infected tissue by gas forming bacteria. The high sugar levels of the diabetics also contribute by facilitating the proliferation of bacteria. The fermentation of sugars enhances the gas production. [4] In non-diabetic patients, higher levels of urinary albumin, lactose, or tissue proteins can result in the formation of gas. [5] It has been proposed that the ischaemia and hypoperfusion of tissues in diabetics impede gas transport from the necrotic tissues and the gas equilibrates with the tissue gas and gradually the gas chamber enlarges [6]. The presence of urinary obstruction increases the tissue pressure, impedes tissue perfusion and enhances the gas formation [6]. Gas, in some of the cases, has been analyzed and was observed to involve varying proportions of hydrogen, carbon dioxide, nitrogen, and oxygen in that order and also trace amounts of ammonia, carbon monoxide and methane in a few cases [2].
Emphysematous Cystitis (EC) was first described in 1671 when a patient complained of passing wind through the urethra [7]. Intramural air was detected in some cases thereafter and it was concluded that both intramural and intravesical air represented the same pathogenetic mechanism. In a series of 135 cases reported over a period of 1956 and 2006, it was seen that the median age was 66 years and at least two-thirds of them were diabetics and women were affected in two-thirds of cases [7]. Patients with urinary obstruction, neurogenic bladder and dysfunctional bladder are more at risk of developing EC. Pneumaturia can be an important symptom associated with fever, cramps in lower abdomen and dysuria. While more than half of them present with these classical symptoms, a few may present with an acute abdomen as shown in the picture. Up to 7% of cases are asymptomatic and may be diagnosed on imaging studies incidentally. Cases of EC have been presented with atypical features of retroperitoneal air as well as peritonitis [5]. Rare cases have presented with subcutaneous emphysema also [8]. Moreover, co-occurrence of EC and Emphysematous Myositis (EM) is infrequently reported, as there is only one reported case in the literature to the best of our knowledge. In their single case report, Bhadada et al. reported EC with EM in an elderly diabetic woman with poorly controlled glycemic status [3]. The reason for the spread of the infection to the muscles as well as the possible route of spread is speculative. It is likely that the gas bubbles passed transmurally to the infra-peritoneal space around the bladder base [5]. It is also possible that the gas bubbles might be carried by the veins draining the bladder into the internal iliac veins and retrogradely to the other draining areas. The vesical veins may even have communications with veins draining the pelvic muscles and causing the retrograde spread of infection. On the other hand, the initial focus of infection in the muscles causing pyomyositis, later spreading to the urinary tract, although possible, was considered less likely. The focus in the muscles would easily spread to the overlying skin and subcutaneous tissue, rather than to the urinary tract and the absence of any such spreading to the skin and the adjacent soft tissue in our patient made this possibility remote.
This case highlights the difficulty in diagnosing urinary infections in haemodialysis patients. Our patient had no urinary symptoms as he had very little urine output . He presented with the sole complaint of debilitating pain in thighs and difficulty in ambulation. It is common in dialysis patients to have very little or no urine output. This causes defunctionalization and inadequate wash-out of the urinary bladder. Many cases of bladder infection complicated by pyocystis have been reported in the literature, where the diagnosis was delayed due to poor urine output [9, 10] The immunocompromised state of dialysis patients coupled with advanced age and poorly controlled diabetes masks fever and other signs of infection, complicating the condition further [9].
The management of EC essentially involves broad-spectrum intravenous antibiotics with concurrent bladder drainage by foley’s catheterization and adequate control of blood glucose levels. Between 10-20% of documented patients with EC require surgical debridement or even cystectomy. The eventual resolution of the collected gas will occur after eradication of the infected organism. EC usually runs a benign course with an overall death rate of 7-10%; this, however, rises to almost 50% when there is concurrent emphysematous pyelonephritis [5, 7, 11]. It is likely that patients with extension of the infection beyond the urinary bladder, as in this case, carry a worse prognosis as it indicates the greater virulence and rapid multiplication of the organism. It is prudent to investigate for urinary obstruction in any case of urinary tract infection and to consider urologic intervention early to prevent complications.
CONCLUSION
To conclude, EC and EPN may rarely present with EM. To the best of our knowledge, this is the second reported case in the world where the patient presented with emphysematous infection in the kidney as well as bladder along with extensive gas in the pelvic muscles. Lower limb pain as an important atypical feature of fatal and extensive urinary infection has been highlighted. It is important that clinicians caring for dialysis patients be aware of this rare presentation of urinary infection.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Informed consent was obtained from the patient.
STANDARD FOR REPORTING
CARE guidelines and methodology were followed.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

