All published articles of this journal are available on ScienceDirect.

A Case of Multiple Wasp Stings Causing Multi-organ Dysfunction Syndrome
Authors Info & Affiliations
Abstract
Wasp stings occur commonly and uncomplicated cases are generally managed at local health centers. Complicated cases are referred to tertiary hospitals for multi-specialty care. We report a case of a 30-year old gentleman from a remote center in Nepal who had multiple wasp stings and developed oligo-anuric acute kidney injury, liver failure, and rhabdomyolysis. He was promptly referred to our hospital after initial resuscitation. At our hospital, he was treated with intensive conventional supportive care and specific organ-supportive care including N-Acetylcysteine infusion and hemodialysis. With the treatment given, the general condition of the patient as well as liver function improved within the first week. However, the recovery of kidney function and urine output lagged behind. The patient showed signs of improvement in kidney function at the end of the third week and completely recovered by the 40th day of treatment.
1. INTRODUCTION
Cases of wasp stings are commonly encountered in Nepal [1-4]. Uncomplicated cases are managed successfully in primary care centers and those with systemic complications are referred to tertiary care hospitals [1-4]. The outcome is variable depending upon factors including the severity of complications, the involvement of different organs, and timely and effective management [1, 3, 5]. Wasp sting causing multi-organ dysfunction is uncommon and carries worse prognosis [5-7]. Mortality among patients who have Acute Kidney Injury (AKI) after wasp sting is said to be as high as 25% [5]. This case report describes a young male patient who presented with multi-organ involvement and made a complete recovery.
2. CASE REPORT
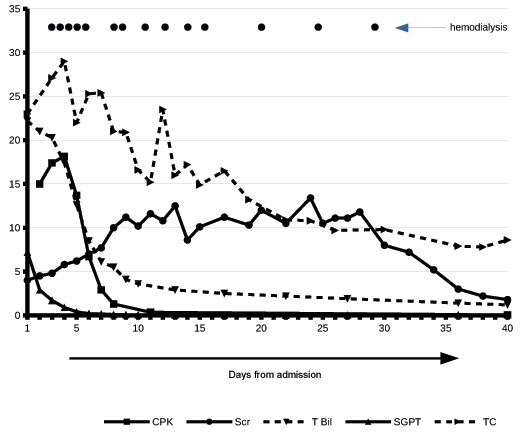
A 30-year old previously healthy gentleman from Khotang was stung by a swarm of wasps (species not identified) one day prior to the presentation. He had severe pain due to the stings. Later that day, he developed jaundice and was noted to have reduced and dark-colored urine. He was initially managed in the local health centre and then referred to our hospital after stabilization. At the time of arrival, the patient was ill-looking and icteric with a puffy face. His blood pressure was 150/90 mmHg with normal heart rate and rhythm. The laboratory investigations showed leukocytosis (Total count: 23000 cells/ml), deranged renal (Serum Creatinine: 4 mg/dl) and liver function tests (Total Bilirubin: 22.9 mg/dl, Serum glutamic pyruvic transaminase 7200 U/L, serum glutamic-oxaloacetic transaminase 2700 U/L), Creatine Phosphokinase (15000 IU/L), and albuminuria without hematuria or casts. Echocardiogram and electrocardiogram were normal. Ultrasonography of kidneys showed diffusely increased cortical echotexture of the kidneys.
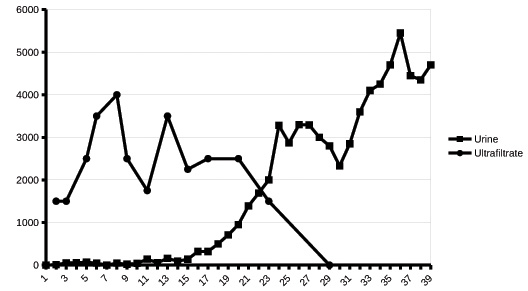
The patient was managed further in the Intensive Care Unit (ICU) with parenteral broad-spectrum antibiotics and fluids. Urine output remained low despite fluid resuscitation and diuretics. The patient remained icteric in the first week of the treatment. He received nutritional support tailored to meet his requirement for recovery and other general supportive care. He received N-Acetylcysteine (NAC) infusion for 72 hours from the second day to intensify recovery of liver function. Hemodialysis was started via a femoral hemodialysis catheter also from the second day of admission as the patient remained anuric and uremic. The hematological parameters, liver function, and general condition of the patient improved in the first week of the treatment (Fig. 1) . He was shifted to the renal ward on the sixth day. In the ward, the patient developed a few episodes of fever and remained oligo-anuric till the end of the third week (Fig. 2). Hemodialysis was continued (Fig. 1) along with antibiotics. Hemodialysis catheter was inserted in the right internal jugular on the eighth day. Gastrointestinal symptoms resolved on Day 12 of admission. The urine output and renal function started to stabilize only in the third week (Fig. 2). Albuminuria resolved on Day 36 of admission. During this period, the patient had received fourteen sessions of hemodialysis (Fig. 1). The patient received inpatient treatment for 40 days out of which he was in ICU for the first 6 days.
At two weeks and two months after discharge on follow-up, the patient was doing well with normal kidney and liver functions.
3. DISCUSSION
Wasp stings cause local and systemic effects primarily due to the wasp venom which contains various active substances including dopamine, adrenaline, hyaluronidase, histamine, serotonin, and phospholipase A. Though a single sting of wasp can cause fatal anaphylaxis, severe complications are usually related to massive envenomation [1, 5] which cause toxin-mediated damages including rhabdomyolysis [4, 5, 8-10], hematological complications [5, 9], liver failure [5, 6], acute kidney injury [1, 2, 4-8, 11-14], myocarditis [5, 13], acute pancreatitis [5, 8], and stroke [5, 16]. The clinical features seen in our patient and the consequences are consistent with multi-organ dysfunction due to wasp sting [5].
AKI due to wasp sting is seen in more than half of the patients who experience multiple wasp stings [5]. AKI is due to direct toxic effect of the venom, ischemic acute tubular injury, and nephropathy due to hemoglobinuria and rhabdomyolysis. Renal biopsy reveals acute tubular necrosis and occasionally acute interstitial nephritis and pigment tubulopathy [6, 11, 12]. Liver injury is rare [5] and the pathogenesis has not been well understood. It could be implicated to direct toxic effect and ischemic injury to the liver.
Treatment of wasp sting is supportive. Adequate fluid resuscitation, maintenance of hemodynamic stability, and proper nutritional support enhance recovery.
As most of the cases with severe complications have acute kidney injury, dialysis (intermittent hemodialysis or peritoneal dialysis) is frequently needed for indications such as electrolyte imbalance, uremia, and fluid overload [5] Plasma exchange with continuous veno-venous hemofiltration has been suggested for the treatment of multiple organ failure after wasp stings [6, 7, 14]. The reported patient received multiple sessions of intermittent hemodialysis which helped in the recovery of the patient.
Intravenous infusion of NAC was given for 72 hours to the patient. NAC infusion is an established treatment for acetaminophen-induced acute liver failure [15, 16], and its use along with conventional treatment has been shown to be beneficial in non-acetaminophen-induced acute liver failure. Our patient received NAC infusion during the initial days of treatment which could have improved the outcome of acute liver failure that the patient had presented with.
The role of steroids in the management of wasp stings other than for initial acute inflammatory reaction is debatable. Our patient did not have features of an acute allergic event but rhabdomyolysis was pronounced. Use of steroid was avoided and did not seem to affect the outcome of the management.
Early referral and management of wasp sting with multi-organ dysfunction improve the outcome.
CONCLUSION
Conventional supportive care along with the intravenous infusion of NAC and intensive hemodialysis support contributed to the successful recovery. The management of such cases with multi-organ involvement should be carried out by a multi-speciality team where dialysis support can be provided till the patient recovers.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Informed consent was obtained from the patient.
STANDARD FOR REPORTING
CARE guidelines and methodology were followed.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

