All published articles of this journal are available on ScienceDirect.

A Comparative Analysis of Norepinephrine with Midodrine/Octreotide in Patients with Hepatorenal Syndrome-acute Kidney Injury
Authors Info & Affiliations
Abstract
Background
Hepatorenal Syndrome (HRS) is a severe complication of end-stage liver disease characterized by functional renal impairment. This study aimed to assess the efficacy of norepinephrine compared to midodrine/octreotide in managing patients diagnosed with hepatorenal syndrome type 1.
Materials and Methods
In this double-blind Randomized Clinical Trial, 50 patients with hepatorenal syndrome type 1 were randomly assigned to the norepinephrine and midodrine/octreotide groups. The norepinephrine group received an initial dose of 1 mg/h (up to a maximum of 4 mg/h) along with daily intravenous injections of 20% albumin (20-40 grams per day) throughout the study period. The control group received midodrine (maximum dose of 15 mg three times a day), octreotide (maximum dose of 200 micrograms intravenously three times a day), and 20 to 40 mg of 20% albumin daily. The primary efficacy measure was the percentage of patients achieving a complete response, defined by the restoration of serum creatinine levels to within 0.3 mg/dl of the baseline by the end of treatment.
Results
There was no significant difference in the rate of complete response between the norepinephrine group (7/25, 28%) and the midodrine/octreotide group (3/25, 12%) (p=0.15). The mortality rate was 10 (40%) in the norepinephrine group and 12 (48%) in the midodrine/octreotide group. Although the mortality rate was higher in the midodrine/octreotide group (12/25, 48%) compared to the norepinephrine group (10/25, 40%), this difference was not statistically significant (p=0.77).
Conclusion
The study findings suggest that the norepinephrine treatment regimen can be as effective as or more effective than the midodrine/octreotide regimen in treating hepatorenal syndrome in cirrhotic patients. Therefore, these two treatment regimens can be used interchangeably.
1. INTRODUCTION
Hepatorenal Syndrome (HRS) arises as a severe complication of end-stage liver disease and is characterized by functional renal impairment. In the setting of liver cirrhosis, HRS manifests as a marked deterioration in renal function, often leading to acute kidney injury (AKI) [1]. The pathophysiology of HRS is complex and multifactorial, bearing intricate interplays between systemic hemodynamic alterations, renal vasoconstriction, and neurohormonal dysregulation [2]. Management of HRS–AKI poses substantial clinical chall- enges, with limited therapeutic options and a pressing need for effective interventions [3]. Historically, initial pharmacotherapeutic approaches have encompassed vasopressors, albumin infusions, and vasoconstrictors, yet the optimal pharmacological strategy remains elusive [4].
In the pursuit of more efficacious treatments for HRS–AKI, the use of midodrine/octreotide regimens has garnered attention as a promising therapeutic avenue [5]. Midodrine, a selective α1-adrenergic agonist, acts to augment systemic vascular resistance, thus ameliorating circulatory dysfunction in HRS patients [6]. In conjunction, octreotide, a somatostatin analogue, complements mido- drine's effects by suppressing splanchnic vasodilation and diminishing portal hypertension [7]. Notably, this combination therapy has demonstrated encouraging outcomes, although its widespread adoption has been hindered by logistical complexities and variability in individual responses [8].
Concurrently, the efficacy of alternative adrenergic agents in the management of HRS–AKI, such as norepinephrine, continues to spur scientific interest [1]. Norepinephrine, a potent α-adrenergic agonist, assumes a fundamental role in modulating systemic vascular resistance and blood pressure, thereby holding potential as an alternative or adjunctive therapy [9]. However, the direct comparison of norepinephrine vis-à-vis the established midodrine/octreotide protocol in ameliorating renal function in HRS–AKI patients remains underexplored [10]. By elucidating the comparative effectiveness and safety profile of norepinephrine against the standard regimen, valuable insights might be obtained, further shaping the landscape of therapeutic modalities for HRS management [11].
The critical implications of the aforementioned therapeutic paradigms for HRS–AKI prompt a meticulous and comprehensive inquiry into the relative merits of these pharmaceutical interventions [12]. Thus, this study aims to seek to address this urgent knowledge gap by conducting a randomized controlled trial, aiming to ascertain whether norepinephrine exhibits comparability or superiority to the midodrine/octreotide combination in enhancing renal function and hemodynamic stability in patients afflicted with HRS–AKI.
2. METHODS
This research employs a double-blind, Randomized Controlled Trial (RCT) design to compare the efficacy and safety of norepinephrine versus the standard midodrine/ octreotide regimen in patients diagnosed with Hepatorenal Syndrome-Acute Kidney Injury (HRS-AKI). The study was conducted at Sayad Shirazi Medical Education and Referral Hospital in Gorgan, Iran, in 2023. The protocol was approved by the Ethics Committee of Golestan University of Medical Sciences (Ethics Committee reference number: IR.GOUMS.REC.1401.374) and registered with the Iranian Registry of Clinical Trials (IRCT20230228057568N1).
The sample size was determined based on the expected effect size (d=1.06) using the results of Gupta et al.'s study [14] in 2018 and using G*Power, 3.1.9.7 software with a statistical power of 95%, and α error probability of 0.05 and a ß error of 0.20, the number of 50 patients (in each group, 25 patients).
Inclusion criteria encompass adult patients (aged 18 and above) diagnosed with hepatorenal syndrome- acute kidney injury as per the established diagnostic criteria based on the 2015 International Club of Ascites (ICA) diagnostic criteria [13]. Exclusion criteria include individuals with contraindications to norepinephrine or midodrine/octreotide, concomitant severe cardiovascular pathology, and preexisting renal replacement therapy. Other exclusion criteria included kidney parenchymal disease or obstructive uropathy in laboratory and ultrasound evaluation, doubling of creatinine level to a value higher than 2.5 mg/dL in 2 weeks or less. Patients who were receiving nephrotoxic drugs having advanced hepatocellular carcinoma, or a known allergy to the study medications were not included in the study. Before enrolling in the study, each patient or their legally authorized representative provided written informed consent. Eligible participants were randomized into either the norepinephrine intervention arm or the midodrine/ octreotide control arm using block randomization with four random block orders: AABB, ABAB, ABBA, BABA, BAAB, and BBAA. Allocation concealment was maintained.
The trial was double-blinded. All patients, the facilitators of the intervention (internal medicine assistants, project manager), and the study outcome investigator (internal medicine assistant) were unaware of the study groups. Only the main executor of the project, the nephrology subspecialist, was informed about the grouping of patients to receive the drug in order to provide direction for treatment or control in the event of possible side effects.
Norepinephrine Arm: Patients assigned to the norepinephrine arm received norepinephrine (Leofed ampoule 4 mg/4 ml, produced in England, imported by Rayan Daro Iranian Company) infusion at standardized dosages for a predefined duration as per the study protocol [13]. Patients with hepatorenal syndrome were treated with norepinephrine at an initial dose of 1 mg/h using continuous injection, which was gradually increased to a maximum dose of 4 mg/h in order to achieve a minimum urine output of at least 400 ml per 12 hours. They received 20% Albumin on the first day of 1 gram per kilogram of body weight and then 20 to 40 grams per day intravenously for up to 14 days, and then clinical and laboratory information in both groups at the beginning and then on days 0 and 14 were checked.
Midodrine/Octreotide Arm: Individuals allocated to the midodrine/octreotide arm underwent administration of midodrine and octreotide according to established dosing regimens. These patients received Midodrine orally with an initial dose of 7.5 mg three times a day, with a dose increase of up to a maximum of 12.5 mg three times a day, together with Octreotide subcutaneously: initial dose 100 μg three times a day and up to 200 μg three times a day and receiving Albumin on the first day of 1 gram per kilogram of body weight. The patients received 20% Albumin, starting with 1 gram per kilogram of body weight on the first day, followed by 20 to 40 grams daily through intravenous administration for up to 14 days. Both groups were assessed for basic, clinical, and laboratory information at the beginning and then again on days 0 and 14.
The primary efficacy endpoint of the study was the proportion of patients who achieved full response, defined as the improvement in renal function, assessed by changes in serum creatinine levels (below 1.5 mg) and urine output (increase in 1-hour urine output above 0.5 ml) over the designated intervention period. The measurement frequency included before the intervention, 0, and 14 days after the intervention.
Additional secondary endpoints encompass hemodynamic parameters, such as mean arterial pressure, creatinine clearance, blood pressure, electrolytes, and vasopressor requirement, as well as adverse event monitoring and 30-day mortality rates. Clinical and laboratory data be systematically collected at pre-determined intervals throughout the study period.
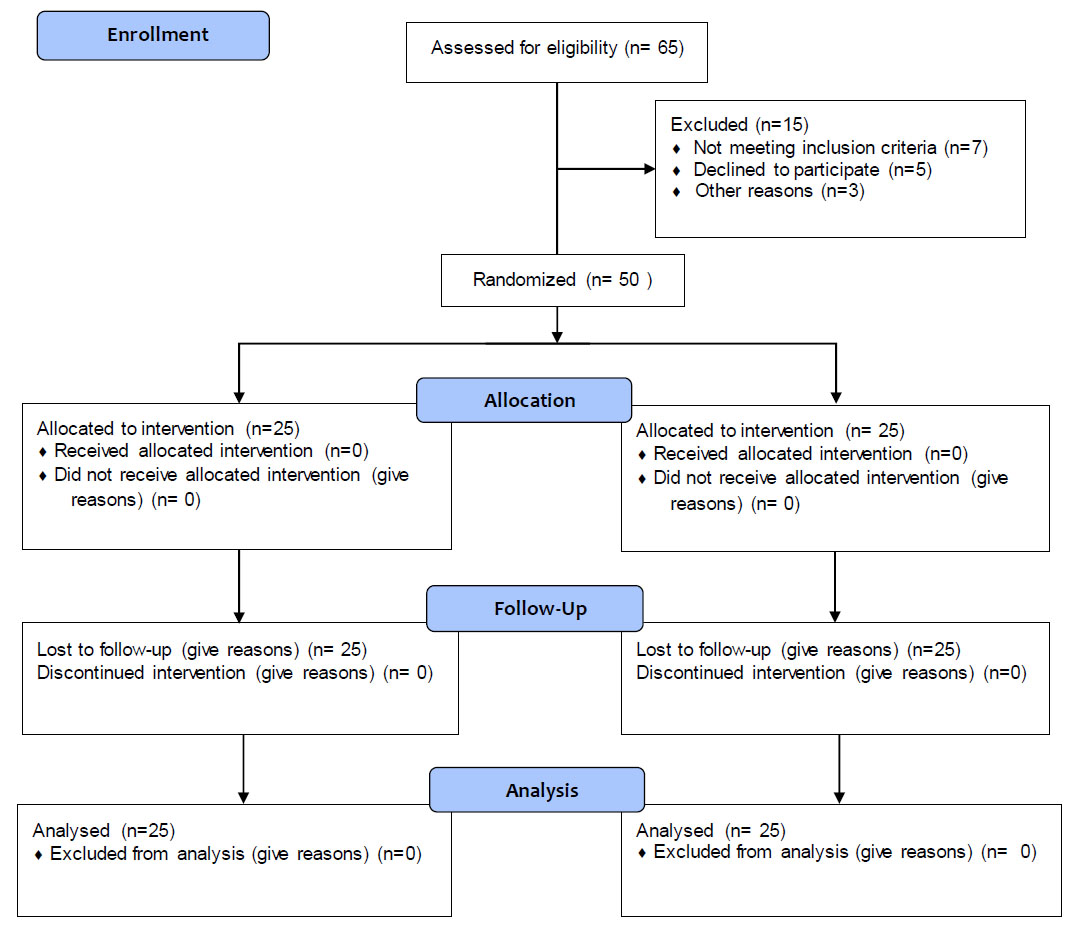
CONSORT flow diagram.
| Variables | Norepinephrine (n=25) | Midodrine/Octreotide (n=25) | p.value |
|---|---|---|---|
| Age (year) | 50.08±10.41 | 52.68±10.43 | 0.38 |
| BMI (kg/m2) | 27.47±4.33 | 28.01±4.12 | 0.45 |
| Gender (n, %) | - | - | 0.55 |
| Male | 15, 60% | 17, 68% | |
| Female | 10, 40% | 8, 32% | |
| Cause of cirrhosis (n, %) | - | - | 0.69 |
| Viral hepatitis | 16, 64% | 19, 76% | |
| Alcoholic liver | 3, 12% | 2, 8% | |
| Wilson's disease | 3, 12% | 1, 4% | |
| Others | 3, 12% | 3, 12% | |
| Serum sodium(mEq/L) | 128.12±8.96 | 126.91±9.01 | 0.39 |
| Serum creatinine (mg/dL) | 3.35±2.12 | 4.12±2.26 | 0.22 |
| Glomerular Filtration Rate (ml/min) | 24.84±15.80 | 25.40±19.45 | 0.13 |
| Urine outpute (ml/day) | 3.60±145.46 | 3.67±208.59 | 0.88 |
| Mean Arterial Pressure (mmHg) | 76.52±8.06 | 78.06±8.04 | 0.06 |
The data was analyzed using a per-protocol approach. Numerical data was presented as mean and standard deviation, while categorical data was reported as frequency and percentage. The Shapiro-Wilk test was used to assess the normality of continuous variables. As the data did not follow a normal distribution, non-parametric tests such as the Mann-Whitney and Wilcoxon-signed ranks tests were employed. For categorical data, the chi-square test was applied with significance set at p<0.05. All analyses were conducted in STATA (version 14, Stata Corp, Texas, USA). Preplanned subgroup analyses were conducted to explore potential differential treatment effects based on specific baseline characteristics, such as severity of liver disease and hemodynamic status (Fig. 1].
3. RESULTS
Table 1 indicates that patients administered norepinephrine and those administered midodrine plus octreotide possessed similar baseline demographic characteristics, as well as clinical and laboratory parameters. The majority of study participants were male (64%) with an average age of 51 years (range 34–72). The underlying cause of liver cirrhosis was identified as viral hepatitis in 35 patients (70%) across both groups.
There was no statistically significant difference in the length of hospitalization norepinephrine (10.12 days) and midodrine/octreotide (9.7 days) groups (range 5–14 days). When defining a complete treatment response as a reduction in creatinine levels to below 1.5 mg/dL post-treatment, it was found that 7 (28%) patients in the norepinephrine group and 3 (12%) in the midodrine/ octreotide group achieved this outcome. However, this difference was not statistically significant, as shown in Table 2. Although the HRS reversal rate was higher in the norepinephrine group than in standard treatment (48% vs. 12%), this difference was not significant (p=0.28). The mortality rate in patients who received norepinephrine was 40%, and in the midodrine/octreotide group, it was equal to 48%. Despite the higher mortality rate in the midodrine/octreotide as a standard treatment, this difference was not statistically significant (p=0.77). There was no statistically significant difference in mortality rate (p=0.25), length of hospitalization (p=0.69) and response to treatment (p=0.88) in men and women patients. The present study did not show any difference in terms of response to treatment in norepinephrine and midodrine/ octreotide groups based on age and gender.
The mean difference between baseline serum creatinine and the level of after treatment in the midodrine/octreotide group was reported respectively, 0.85±0.19 and 0.58±0.34 mg per dL. Comparison of the difference in creatinine levels before and after treatment was not statistically significant (p=0.36). Also, the comparison of the level of creatinine in each group before and after the treatment indicated a significant decrease in the midodrine/octreotide group (P=0.004).
Regarding Creatinine Clearance (CrCl), the mean Glomerular Filtration Rate (GFR) after the intervention in the norepinephrine group was 40.24±22.30 and in the midodrine/octreotide group 24.84±17.77 ml per min. Still, the mean difference of GFR before and after the intervention was not significant between the two study groups (p=0.96).
4. DISCUSSION
The results of the presented randomized controlled trial provide a compelling insight into the therapeutic paradigms for managing hepatorenal syndrome-acute kidney injury (HRS-AKI) and offer noteworthy implications for clinical practice. The study aimed to assess the comparative efficacy of norepinephrine against the standard midodrine/octreotide regimen, and the findings bring to light valuable observations regarding treatment response and mortality outcomes among patients afflicted with HRS-AKI.
The investigation revealed that the rate of full response, a pivotal measure of treatment effectiveness, demonstrated no statistically significant disparity between the norepinephrine and midodrine/octreotide groups. Notably, the full response rate in the norepinephrine cohort stood at 28%, which contrasted with the 12% rate observed in the midodrine/octreotide arm. Although this disparity did not reach statistical significance (p=0.15), the observed trends underscore the potential comparability of norepinephrine with the established therapeutic combination, shedding light on the equipoise of these treatment modalities in achieving full renal functional recovery. The comparable response rates pose critical implications for the selection of therapeutic regimens, prompting a reevaluation of the clinical utility of norepinephrine and the midodrine/octreotide protocol in the management of HRS-AKI [14-16].
| Variables | Norepinephrine (n=25) | Midodrine/Octreotide (n=25) | p.value |
|---|---|---|---|
| Full response to treatment | 7, 28% | 3, 12% | 0.157 |
| Length of hospitalization (day) | 10.12±2.74 | 9.72±2.59 | 0.59 |
| Mortality (n, %) | 12, 48% | 10, 40% | 0.77 |
| HRS reversal | 7, 28% | 3, 12% | 0.28 |
| Serum sodium(mEq/L) | 6.90±8.40 | 2.00±5.60 | 0.08 |
| Serum creatinine (mg/dL) | 0.58±0.34 | 0.58±0.19 | 0.36 |
| Glomerular Filtration Rate (ml/min) | 8.53±3.40 | 6.72±2.03 | 0.96 |
| Urine outpute (ml/day) | 8.60±28.56 | 25.75±19.28 | 0.29 |
| Systolic blood pressure (mmHg) | -6.00±15.25 | -2.90±7.68 | 0.51 |
The present study did not show any difference in terms of response to treatment in norepinephrine and midodrine/octreotide groups based on age and gender. Other studies also did not show a difference in the results of the treatment among the vasoconstrictor drugs used in the treatment of hepatorenal syndrome according to the gender and age of the patient, and therefore, it seems that these two factors do not affect the choice of the type of treatment [10, 17].
Tavakoli et al.'s study [18] found complete response to treatment in 73% of patients in the norepinephrine group and in 75% of patients in the midodrine/octreotide group. In the study of El-Desoki et al. [10], the rate of complete response to treatment was 57.6% in the norepinephrine group and 20% in the midodrine/octreotide group, and these results significantly supported the treatment with norepinephrine.
Furthermore, an examination of mortality rates across the two intervention arms yielded intriguing insights. Although a higher mortality rate was observed in the midodrine/octreotide group (48%) compared to the norepinephrine group (40%), this difference did not bear statistical significance. In the study of El-Desoki et al. [10], 11 patients (42.30%) in the norepinephrine group and 6 patients (24%) in the midodrine/octreotide group survived, with no statistically significant difference. The median survival times were 16 days and 11 days, respectively.
The results of this study accentuate the need for a rigorous evaluation of therapeutic strategies in HRS-AKI, ascertaining their impact on not only renal function but also patient survival. The comparable treatment response rates and mortality outcomes between norepinephrine and the established midodrine/octreotide protocol underscore the complexity of therapeutic decision-making, paving the way for individualized approaches in HRS-AKI management [15, 19]. A contextual understanding of patient- specific variables, disease severity, and hemo- dynamic status is imperative in guiding treatment selection, highlighting the intricacies surrounding the optimization of therapeutic interventions in HRS-AKI.
In the context of hepatorenal syndrome, the optimal treatment often involves liver transplantation, particularly for patients who are deemed suitable candidates for transplantation [20]. However, it is crucial to acknowledge that not all patients are viable candidates for this definitive intervention, thereby necessitating alternative therapeutic strategies. One notable pharmaceutical option, terlipressin treatment, has shown promise in the management of hepatorenal syndrome [21]. Nonetheless, despite its potential benefits, the availability of terlipressin treatment remains a challenge in certain healthcare settings, limiting its widespread use and accessibility to patients in need. The complex management of hepatorenal syndrome emphasizes liver transplantation as the primary treatment for suitable candidates. The limited availability of terlipressin underscores the need to improve treatment options for patients ineligible for immediate transplantation. Bridging gaps in care delivery is crucial to meet the therapeutic needs of hepatorenal syndrome patients, particularly those not eligible for transplants.
CONCLUSION
The findings of this study indicated that the Norepinephrine treatment regimen can be as effective as or more effective than the midodrine/octreotide treatment regimen in the treatment of hepatorenal syndrome in cirrhotic patients, and these two treatment regimens can be used interchangeably. The outcomes of this study propel the need for future research endeavors delineating the determinants of treatment response and mortality in HRS-AKI, weaving in diverse patient populations and elucidating the nuances of therapeutic efficacy. Additionally, long-term follow-up studies are warranted to unravel the sustained impact of norepinephrine and midodrine/octreotide regimens on renal recovery and patient survival.
AUTHORS’ CONTRIBUTION
It is hereby acknowledged that all authors have accepted responsibility for the manuscript's content and consented to its submission. They have meticulously reviewed all results and unanimously approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| HRS | = Hepatorenal Syndrome |
| AKI | = Acute Kidney Injury |
| RCT | = Randomized Controlled Trial |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The protocol was approved by the Ethics Committee of Golestan University of Medical Sciences (Ethics Committee reference number: IR.GOUMS.REC.1401.374) and registered with the Iranian Registry of Clinical Trials (IRCT20230228057568N1).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committees and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Before enrolling in the study, each patient or their legally authorized representative provided written informed consent.

