All published articles of this journal are available on ScienceDirect.

Study on Echocardiographic Parameters of Left Ventricular Dysfunction Before and After Initiation of Maintenance Hemodialysis in End-stage Kidney Disease Patients
Authors Info & Affiliations
Abstract
Background
Chronic kidney disease (CKD) is a global health issue, resulting in approximately one million fatalities annually. Cardiovascular complications continue to be a significant contributor to mortality, and this was a study conducted to assess the changes and risk reduction of cardiovascular complications after initiating maintenance hemodialysis.
Objectives
To study echocardiographic changes before and after initiation of dialysis in ESKD patients with a simple non-invasive bedside assessment of 2D Transthoracic Echocardiography (TTE).
Methodology
It was a cross-sectional observational study. All the patients included in the study either attended the out-patient department or were admitted at Sri Ramachandra Institute of Higher Education and research, over a period of 3 months. The study included patients aged >18 years who had given written consent and fulfilled the KDIGO (Kidney diseases improving global outcomes) criteria of CKD stage 5 requiring hemodialysis initiation.
Results
A total number of 57 patients were included in the study. The mean age was 46 ± 10 years. Among co-morbidities, 53 patients (93%) were hypertensive and 44 patients (77.2%) also had diabetes mellitus. The mean LVIDs (Left ventricular end-systolic diameter) was 32±3mm (pre-HD initiation) as compared to 31±3.3mm 3 months post-HD(hemodialysis) initiation. The mean EF (ejection fraction) pre-HD was 42% and 48% after 3 months of HD.
Conclusion
We advocate for a two-fold approach. Firstly, we recommend that all end-stage renal disease patients undergo an echocardiogram screening before commencing dialysis. Secondly, we propose that these patients should be re-evaluated after receiving adequate hemodialysis.
1. INTRODUCTION
Chronic Kidney Disease (CKD) is a predominant debilitating problem all over, draining all the resources and also increasing the financial burden for a number of families. These patients are at an increased risk of cardiovascular diseases (CVD), and the risk of developing these diseases is 3 times more in end-stage renal disease (ESRD) patients on maintenance hemodialysis (HD) [1-3]. It applies to almost 44% of mortality in all ESRD patients on dialysis.
Congestive Heart Failure is responsible for approximately 15% of deaths and substantial non-fatal dialysis-associated morbidity [1, 4].
In dialysis patients, left ventricular hypertrophy and dilated cardiomyopathy is pronounced mostly related primarily to prolonged hypertension and extracellular fluid overload; also, anemia and iatrogenic AV fistula lead to heart failure. Arteriovenous (AV) fistula, increases stroke volume load on the left ventricle, which causes LVH and may result in LV systolic and diastolic dysfunction with time. In addition to this, the presence of an AVF reduces systemic vascular resistance [2, 4]. The diagnosis of LV abnormalities by Doppler echocardiography is an important step for the characterization of individuals with higher CV risk. To estimate the prognostic impact and to bring about therapeutic early interventions, we studied the echocardiographic changes in dialysis patients with a simple noninvasive bed-side assessment of 2D Trans- thoracic Echocardiograpgy (TTE).
2. MATERIALS AND METHODS
All the patients included in the study either attended the OPD or IP admission at Sri Ramachandra Institute of Medical Science over a period of 3 months. The study included patients aged >18 years who had given written consent and fulfilled KIDGO criteria of CKD V requiring hemodialysis initiation. The study was conducted between December 2021 to March 2022
The patients who did not give written informed consent, and have already undergone hemodialysis, mental illness, history of CAD and other cardiac disorders (e.g.: valvular heart disease, congenital heart disease) were excluded from the study. All the patients included were on twice-weekly hemodialysis sessions.
All the patients needing HD initiation were first subjected to a 2D Echocardiographic study and were again subjected to 2D echocardiographic after 3 months of maintenance hemodialysis to assess the echocardiographic profile.
Patients diagnosed with anemia (males Hb<13.5gm% ; females hemoglobin <12.5gm/dl) were started on adjuvant therapy for anemia (iron supplements and erythropoietin therapy) after detailed evaluation
Hypertension was defined as blood pressure >140/80mmHg and patients were initiated on appropriate anti-hypertensives under serial BP reading monitoring.
While assessing the echocardiographic profile:
The following parameters were measured:
a) Left ventricular end-diastolic diameter (LVIDed)
b) Left ventricular end-systolic diameter (LVIDes)
c) Ventricular septum thickness (IVSTed)
d) Ejection Fraction
e) Posterior Wall Thickness in Diastole
Cardiac abnormality was defined according to the American Society of Echocardiography (ASE) and European Society of Cardiology guidelines with minor modifications to account for kidney failure patients. For the purpose of this study, five parameters were utilized to assess cardiac function. Left ventricular hypertrophy (LVH) was defined as a left ventricular mass index (LVMi) greater than 100 g/m2 for women and greater than 130 g/m2 for men. Increased left ventricular volume index (LVVi) was defined as greater than 86 ml/m2 end-diastolic volume or greater than 37 ml/m2 end-systolic volume [3].
We calculated LVH according to the following:
1. LV mass = 1.05 ([LVIDD + PWTD + IVSTD] 3 - [LVIDD] 3) g
Where: LVIDD = Left Ventricular Internal Diameter in Diastole
PWTD = Posterior Wall Thickness in Diastole
IVSTD = Interventricular Septum Thickness in Diastole
2. EF (%) = SV/EDV *100
Where the stroke volume is given by,
SV= EDV- ESV
3. Left ventricular fractional shortening: fractional shortening was calculated as
FS (%) = (LVDd-LVDs)/LVDd × 100
2.1. Statistical Analysis
The results of the study are analysed using spas Software.
The data is expressed in percentage, mean and standard deviation p-value for pre-test - 5.72 and post-test - 4.56 is considered Statistically significant.
| Baseline Characteristics | Mean |
|---|---|
| Age | 46 ± 10years |
| Sex | Males 49 ; Females – 8 |
| Systolic BP | 150±7.2mmHg |
| Diastolic BP | 87±12.1mmHg |
| Hemoglobin | 8.8±2.3gm% |
3. RESULTS
A total of 67 patients were enrolled, but 10 patients were lost to follow up, and hence a total number of 57 patients were included in the study. The mean age was 46 ± 10 years. The number of males was 49 (85.9%) and 8 (14%) female patients. Among co-morbidities, 53 patients were hypertensive and 44 of the 53 patients also had additional type II diabetes mellitus (Figs. 1-5) and (Table 1).
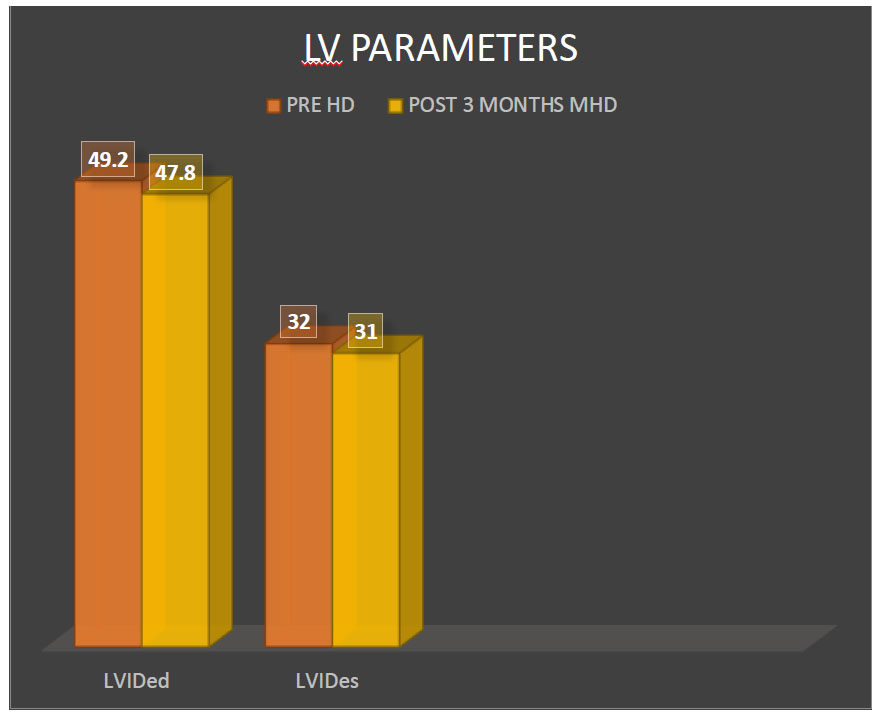
Left ventricular end diastolic and systolic diameter. Pre-hemodialysis and 3 months post hemodialysis.
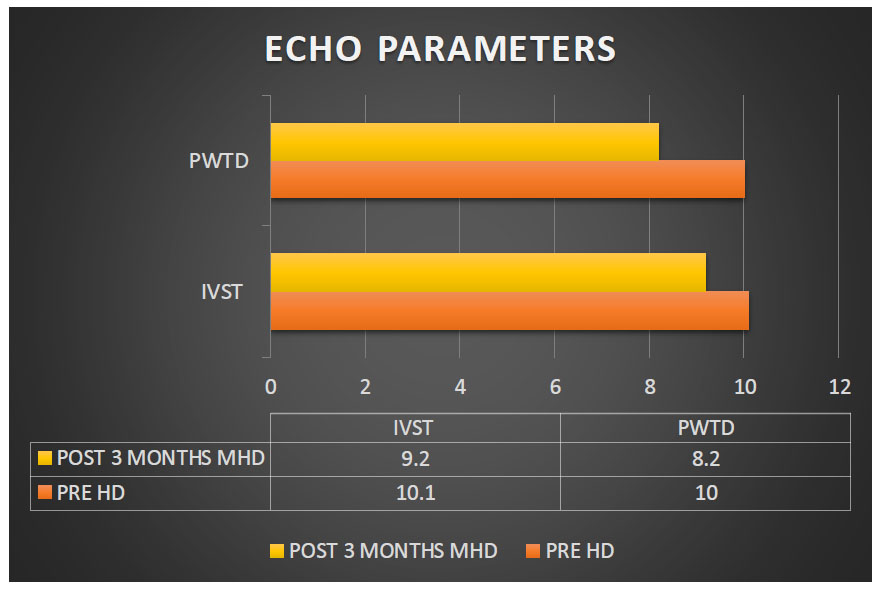
Comparison of Interventricular septal thickness and posterior wall thickness in diastole (measured in MM).
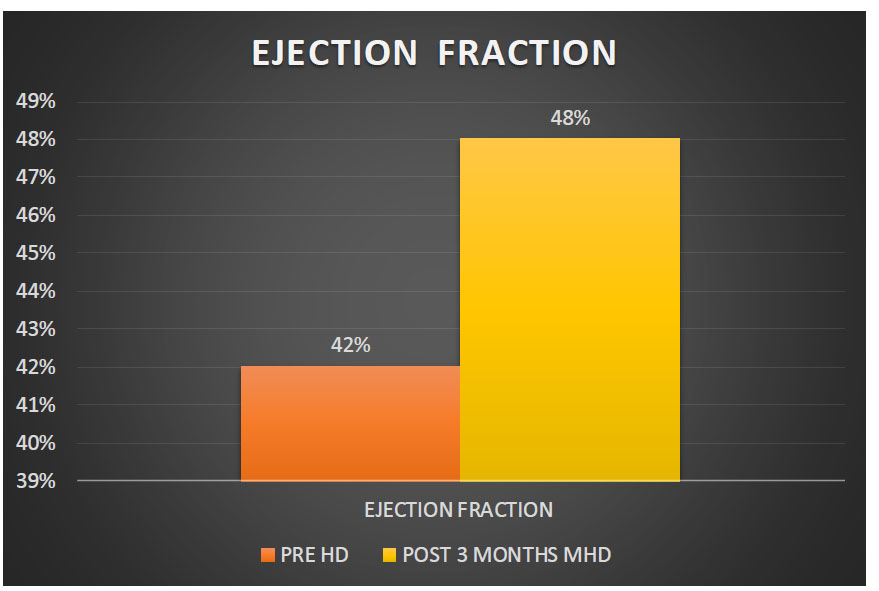
Comparison of ejection fraction(EF).
Comparison of left ventricular shortening.
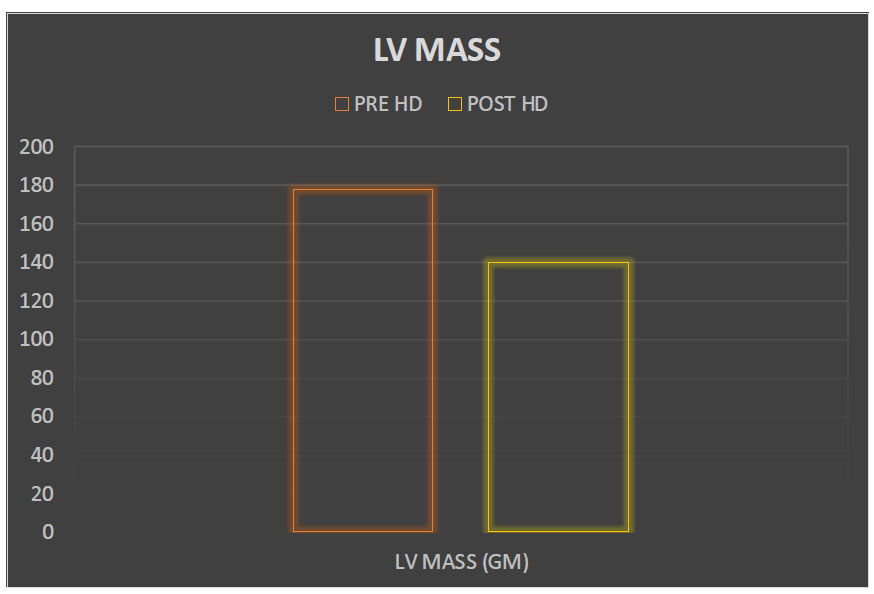
Comparison of LV mass pre and post-HD was calculated. A reduction in LV mass post-adequate dialysis was noted.
The mean LVIDed (left ventricular end-diastolic diameter) was 49.2±1.2mm (pre HD initiation) and post 3 months maintenance HD- 47.8±2.5mm. The mean (Left ventricular end systolic diameter) LVIDes - 32±3mm (pre HD) as compared to post-HD - 31±3.3mm.
There was a significant reduction in the end diastolic and systolic diameter observed post 3 months of twice-weekly maintenance hemodialysis. It was statistically significant (p-value -0.0031).
When these values were compared prior to initiation of hemodialysis and post 3 months of maintenance hemodialysis (twice weekly), there was a statistically significant reduction in both parameters (p-value <0.004 and <0.003, respectively).
We noticed a statistically significant improvement in the ejection fraction in the patients after 3 months of adequate hemodialysis. The mean EF pre-HD was 42% and post HD-48%. (p-value <0.003).
No significant difference was seen in LVFS values pre- and post-hemodialysis.
We get the percentage of size differences of the left ventricle as a parameter of how well the left ventricle is contracting itself and, therefore, reduces the size during systole. Values > 28% are considered to be normal.
The importance of LV mass lies in the fact that it is an independent risk factor for cardiovascular morbidity.
4. DISCUSSION
Left ventricular (LV) malfunction serves as an early indicator of cardiovascular disease (CVD) and subse- quently results in left ventricular hypertrophy (LVH) over time [4]. Moreover, within the hemodialysis (HD) population, cardiomyopathy arises from factors such as obstructed coronary arteries, diminished coronary reserves, and structural abnormalities in the left ventricle due to increased volume and pressure loads [5-7]. When attempts to decrease left cardiac preload are not undertaken, an activation of adaptation in the left ventricle is triggered. This results in a reduction of capillary density, diastolic dysfunction, disruptions in intraventricular conduction, and dilation, and an increase in compensatory hypertrophy [6, 8]. Echocardiography stands as the foremost diagnostic method for identifying abnormalities in cardiac structure and function [8-10]. Hence, we used 2D Thransthoracic echocardiography to assess the echo parameter changes pre and post-HD. In our study, 85% were male patients and 92% were hypertensive and 83% of the study population had diabetes mellitus in addition to systemic hypertension. Ladha et al. documented a higher prevalence of LVH among dialysis patients at 78% and our study showed a similar incidence of 76.8% of patients with LVH. As there is a progressive decline in glomerular filtration rate (GFR), there is an increase in LVH and diastolic dysfunction, with the increased incidence of congestive heart failure [9, 11]. In our study, 27% had diastolic dysfunction and 19% had systolic dysfunction. Post 3 months of adequate dialysis, there was a significant reduction of LVH and also improved ejection fraction. On follow-up, there was a reduction of antihypertensive requirement in 4 patients from 3 to 2 antihypertensives after adequate hemodialysis. Our study shows similar results to other studies. Patients with poor EF have a higher risk of mortality and are more prone to valvular heart diseases, as observed by Yamada et al., we encountered no mortality or valvular heart diseases in our study, probably due to shorter duration of follow-up. In a cohort of patients who had experienced myocardial infarction and were part of the VALIANT trial, an association was found between poor kidney function and a smaller left ventricle, larger volume in the left atrium, and a higher index of left ventricular mass [12, 14]. However, when looking at hypertensive patients with asymptomatic diastolic dysfunction from the VALIDD and EXCEED trials, there was no observed link between the estimated glomerular filtration rate (eGFR) and echocardiographic assessments of left ventricular structure and function [13-15]. We did not find any significant difference in the LVFS pre and post hemodialysis.
The limitations of our study included study duration for follow-up ECHO was 3 months and other markers of inflammation could not be taken into account.
CONCLUSION
The above study suggests and shows significant improvement in echocardiographic parameters in main- tenance hemodialysis patients, with improvement in quality of life with fewer complications during dialysis and less risk for CV diseases. Echocardiography is a widely available non-invasive bedside assessment for CVD prognosis and early intervention if warranted. We recommend all ESRD patients, prior to initiation of dialysis, should undergo ECHO screening and also should be reassessed after adequate good hemodilaysis.
AUTHOR’S CONTRIBUTION
It is hereby acknowledged that all authors have accepted responsibility for the manuscript's content and consented to its submission. They have meticulously reviewed all results and unanimously approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| CKD | = Chronic kidney disease |
| TTE | = Transthoracic Echocardiography |
| CVD | = Cardiovascular Diseases |
| ESRD | = End-stage Renal Disease |
| HD | = Hemodialysis |
| LVH | = Left Ventricular Hypertrophy |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethics approval was obtained from the Institutional Ethics Committee, Sri Ramachandra Medical Institution of Higher Education and Research Centre, Chennai. India
Ethics approval number – CSP-MED/23/NOV/96/292.
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committees and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Informed consent has been taken from the participants involved in the study.

