All published articles of this journal are available on ScienceDirect.

LEARNING FROM IMAGES Staghorn Calculi
Staghorn calculi can damage the kidney and/or lead to life threatening urosepsis. On plain radiograph, vast majority of staghorn calculi are radio-opaque. Associated caliceal dilatation with staghorn calculi is identified on computed tomogram (CT) scan as shown in Fig. (1). A CT scan of a complete staghorn calculus with 3D volume rendered image is shown in Fig. (2).
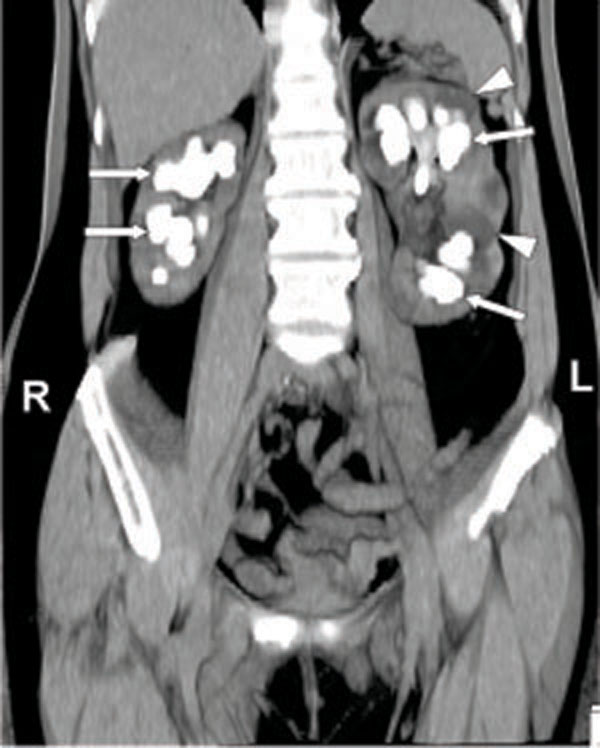
Bilateral staghorn calculi in a 50 year old female patient with recurrent urinary tract infection. Coronal maximum intensity projection non contrast CT scan image shows calculi filling the renal calices (arrows). Dilated calices are also present in the left kidney (arrowheads).
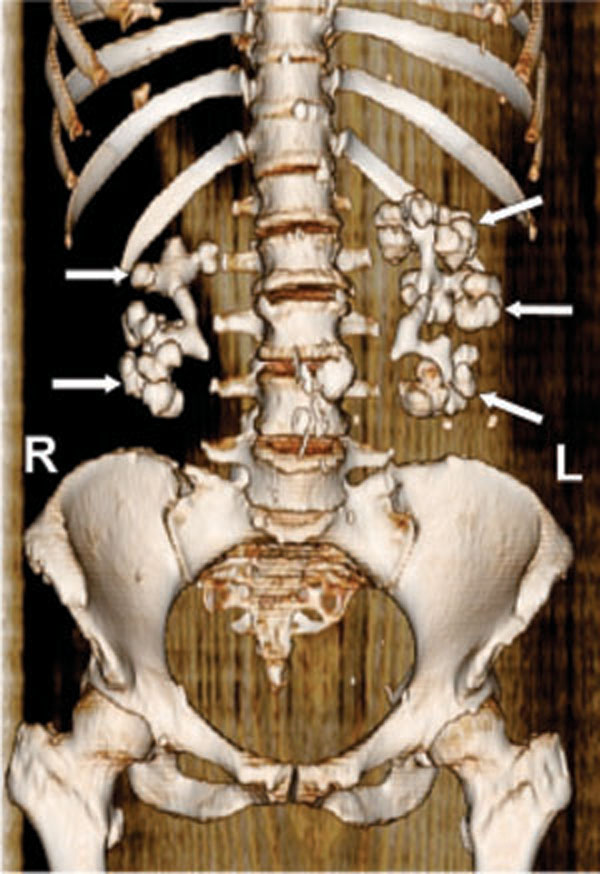
3D volume rendered image shows calculi forming a cast of the renal calices and pelvis (arrows), simulating excretory phase pyelogram.
The term “partial” or “complete” staghorn calculus designates a branched stone that occupies part or the entire pelvicaliceal system. Approximately 70% of staghorn calculi are composed of mixtures of magnesium ammonium phosphate (struvite) and/or calcium carbonate apatite. Cystine, uric acid and calcium oxalate/phosphate components rarely form staghorn calculi. The clinical characteristics that are commonly associated with staghorn configuration include: women, neurogenic bladder, ureteral diversion to ileum and recurrent urinary tract infection with urease producing bacteria (such as Proteus, Klebsiella, Pseudomonas and Enterobacter). The generation of ammonia and hydroxide from urea by these bacteria creates an alkaline environment that promotes crystallization of struvite in the urine [1].
Treatment involves complete removal of the stone, as small residual fragments can act as a nidus for infection and recurrent stone formation. The American Urological Association (AUA) has proposed four modalities as potential therapeutic alternatives for staghorn calculi: 1. Percutaneous nephrolithotomy (PNL) monotherapy; 2. Combination of PNL and shock-wave lithotripsy (SWL); 3. SWL mono-therapy; and 4. Open surgery. AUA recommends nephrec-tomy for non-functioning kidney with staghorn calculi and avoid SWL for staghorn formed predominantly with cystine [2].
CONFLICT OF INTEREST
The authors confirm that this article content has no conflicts of interest.
ACKNOWLEDGEMENTS
Declared none.

