All published articles of this journal are available on ScienceDirect.

Subclavian or Internal Jugular Tunneled Dialysis Catheter: Can we Divulge the Location?
A reliable and safe vascular access is critical for providing life sustaining hemodialysis therapy to patients with end stage renal disease (ESRD). Although a permanent arteriovenous access such as an arteriovenous fistula or arteriovenous graft is preferred, the United States Renal Data System (USRDS) data reports that nearly 80 percent of incident hemodialysis patients initiate treatment with a central venous catheter [1]. While the ability to use a tunneled hemodialysis catheter (THDC) immediately after placement is a significant advantage, it is often offset by a wide array of disadvantages such as increased likelihood of catheter related blood stream infection, catheter thrombosis, and fibrin sheath formation leading to catheter dysfunction resulting in a higher incidence of associated morbidity and mortality. In addition, there is a substantial risk of central venous stenosis (CVS) or occlusion, specially in the setting of long-term use of multiple catheters [2]. The true incidence and prevalence of CVS in the ESRD population are unknown; however, it has been reported to be as high as 30-50% with subclavian vein catheters and potentially the lowest (around 10%) with an internal jugular vein (IJ) THDC [2, 3]. Moreover, placement of THDC can permanently compromise future access placement in the ipsilateral extremity.
Kidney Dialysis Outcome and Quality Initiative (KDOQI) guidelines recommend use of right internal jugular vein as the preferred site for THDC placement. Based on expert consensus, the catheter tip is usually positioned in the mid – to lower right atrium (Fig. 1). However, there is no agreement with regard to catheter exit site and it often varies depending on the patient’s gender, body habitus and amount of soft tissue in the neck and chest region, and the type and length of the catheter. In general an exit site for an IJ THDC is midway between the humeral head and sternal head of the clavicle, roughly one to two centimeter below the clavicle (Fig. 2). The goal is to achieve a smooth wide curve of the segment in the subcutaneous tunnel between the venotomy and exit site [4]. The catheter cuff should be preferably placed below the clavicle, about two centimeters proximal to the exit site.
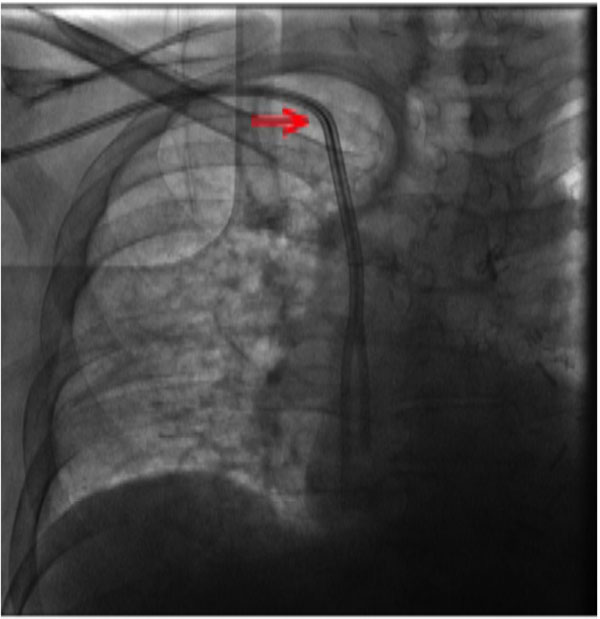
Fluoroscopy appearance of right internal jugular tunneled dialysis catheter with the tips in mid–right atrium. The catheter travels above the clavicle before it enters the central veins (red arrow).

Recently placed right internal jugular tunneled dialysis catheter with exit site in the infraclavicular region about 2 cm below the clavicle.

Multiple scars in the infraclavicular region (red arrow) from previous catheter placements. Small collateral veins (yellow arrow) are visible over the pectoral region.
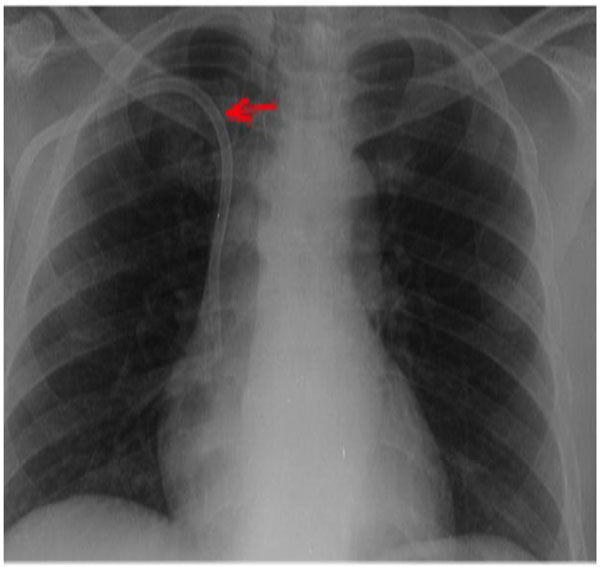
A portable CXR confirming the catheter overlapping the clavicle (red arrow) confirming its position in the right subclavian vein.

A subclavian tunneled catheter is shown by red arrow. A venogram through the right brachial vein revealed occlusion of the right subclavian vein with multiple collateral veins (yellow arrow) draining contrast into the superior vena cava.
Because of the higher incidence of associated CVS, subclavian THDC is seldom seen in clinical practice. Although, the subclavian vein may be accessed by supraclavicular or infraclavicular approaches; the later approach is utilized widely, since the time when it was first described by Aubaniac's in 1952 [5]. Arguably, the supraclavicular route is thought to have several advantages such as, a well-defined insertion landmark (the clavisternomastoid angle), proximity to skin, straighter path to the superior vena cava and less risk of pneumothorax [6]. However, this approach is not widely used partly because, limited experience and training, difficulty in identifying the landmarks along with the risks related to blind insertion technique. Moreover, the utility of supraclavicular approach for a tunneled dialysis catheter placement is unknown. The term subclavian catheter will refer only to infraclavicular subclavian approach for the remainder of this article [7]. An Internal jugular THDC is often misinterpreted as a subclavian THDC. This common clinical error is often linked to lack of knowledge and reluctance or unwillingness to perform a simple physical examination. A concise, quick, and meticulous assessment using basic physical examination skills can help distinguish between an IJ and a subclavian THDC. On inspection, the exit site of a subclavian catheter is often lower and lateral compared to an IJ THDC (Fig. 3). On palpation the subclavian catheter is often felt as “vanishing under the clavicle” whereas the IJ catheter travels over the clavicle into the venotomy site at the base of the neck. A chest radiograph, although not necessary, can reveal the subclavian catheter either overlapping the clavicle or traveling below the clavicle (Fig. 4), while an IJ catheter will travel above the clavicle in to the cervical region. It should be noted that a subclavian catheter placed by a supraclavicular approach may mimic an IJ THDC exam findings. Besides the usual stigmata of CVS namely extremity swelling, presence of collateral veins in the chest, multiple scarring from prior THDC placements; a subclavian THDC itself, could be an ominous sign indicating lack of other commonly available venous THDC placement sites (i.e. internal jugular vein) (Fig. 3). A venogram can be performed to confirm the diagnosis of CVS as shown in Fig. (5).
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

