All published articles of this journal are available on ScienceDirect.

Sexual Function and Correlates in Women Undergoing Maintenance Hemodialysis in Cameroon: A Multi-centric Study
Authors Info & Affiliations
Abstract
Purpose of The Study:
The aim of this study was to describe sexual function disorders and investigate associated factors in women on maintenance hemodialysis in Cameroon.
Methods:
This was a cross-sectional study of three months duration (August-October 2014) in adult women on maintenance hemodialysis (HD) at three HD facilities in Cameroon. Patients with active psychiatric disease, infection or uncontrolled congestive heart failure were excluded. We use the Rosen questionnaire for evaluating female sexual function (FSFI), the Beck depression Inventory (BDI) and the short form (SF-36) of WHOQOL- BREF questionnaire to evaluate the quality of life (QOL). Logistic regressions were used to investigate the predictors of sexual function disorders.
Results:
We included 52 women with the mean age of 38±13 years (min-max: 18-69), with 31 (62%) being of child-bearing age (18-44 years). All participants had at least one sexual function abnormality including sexual dysfunction (75%), abnormalities of the menstrual cycle (83%), and sexual inactivity (30%). In women of child-bearing age, reported menstrual disorders were: irregular menses (45%), non-gravid amenorrhea (40%), oligo-menorrhea (25%), poly-menorrhea (25%), metrorrhagia (6%), and menorrhagia (3%). Ten of the 31 women had more than one menstrual disorder. Sexual dysfunction included: decreased sexual desire (56%), decreased sexual arousal (39%), decreased vaginal lubrication (49%), and failure to achieve orgasm (46%), sexual dissatisfaction (51%), and dyspareunia (36%). Advanced age (p = 0.0046), depression (p<0.0001), anemia (p=0.0005) and poor quality of life were negatively associated with sexual dysfunction. Sexual inactivity (p = 0.035) was equally associated with poor quality of life.
Conclusion:
Our results suggest that disorders of sexual function are common in women on maintenance hemodialysis, and are associated with depression, poor quality of life, advanced age, and anemia.
I. INTRODUCTION
Advances in medical care have improved survival among patients on maintenance hemodialysis (HD) [1]. Although life-preserving, HD is associated with a high symptom burden, and impaired quality of life [2, 3]. Depression, pain, itching, impaired sleep, and fatigue are commonly reported by people undergoing maintenance HD [4, 5]. Sexual dysfunction may also contribute to the symptom burden of Chronic Kidney Disease (CKD). Overall, three quarters of men on HD experience erectile dysfunction [6]. In contrast to the increasing awareness of erectile dysfunction (6), sexual dysfunction in women with CKD is less well known. Studies in Europe, America and Asia have reported the prevalence of sexual dysfunctions in women on HD to range between 80 and 100% [7-9]. Data from sub-Saharan Africa (SSA) is lacking. The number of patients on maintenance HD is gradually increasing in SSA with a corresponding increase in survival. Sexual behavior is partly influenced by social norms. Therefore, data from other parts of the world may not be applicable to SSA. The aim of this study was to describe disorders of sexual function and investigate the associated factors in women on maintenance HD in Cameroon.
II. PATIENTS AND METHODS
Study Setting
The study took place in three HD facilities in Cameroon. All were public facilities, subsidized by the government, and offering only two dialysis sessions per week.
- The HD Unit of General Hospital of Yaoundé which is considered as the reference center of in the country has 18 functional machines and provides dialysis care to about 120 patients. The staff of the unit includes nephrologists and qualified support staffs.
- The Bamenda and Buea HD units are both regional centers, with 08 machines each and provide ongoing care to about 40 to 50 patients. These units are headed by trained general practitioners.
Study Population
Women aged 18 years and above on maintenance HD for at least three months at any of the three participating units were eligible for the study. After information and explanation of the aim of the study, a consent form was signed by all patients willing to participate. Participants were enrolled consecutively between August and October 2014. Those with active psychiatric disease, infection, uncontrolled congestive heart failure were excluded. Biochemical and hematologic data used were the average results of measurements within the preceding six months. Relevant socio-demographic and clinical data were extracted from the patients’ records.
Procedure
Patients were approached in the participating centers during HD sessions. Ethics approval was obtained from local ethics committees and the administration of the different hospitals. Three questionnaires were self-administered with when needed the assistance of the investigator. (1) the Index of Female Sexual Function (IFSF) to assess sexual function; (2) the Beck Depression Inventory (BDI) to rate the severity of depressive symptoms; and (3) the 36-item Short Form Health Survey Questionnaire (SF-36, Taiwan Standard Version1.0) to assess the quality of life. All the questionnaires were made available in their validated French and English version.
- The FSFI [10] is a 19-item questionnaire that assesses 6 distinct domains of sexual function including desire, arousal, lubrication, orgasm, satisfaction, and pain. Scores on the individual domains are computed by summing responses on specific groups of questions and multiplying by a domain factor. The responses were graded on a scale of 1 (almost never or never) to 5 (almost always or always). The highest possible total score was 45 (range 5 to 45), and the lower scores represented lower sexual function. We used a total FSFI score of 28 or lower to indicate the presence of sexual dysfunction.
- The BDI is a standard self-administered questionnaire used to screen patients for depression. It is a valid and reliable international questionnaire for measuring depression and has been used in the assessment of depression in End Stage Renal diseases (ESRD) [5, 13]. In the present study the version with 20 questions was used. Achieving higher score meant more depression. Score less than 15 was considered normal.
- The SF-36 is an instrument commonly utilized to measure the quality of life in the general [2, 14] and uremic populations [3]. It includes eight scales: physical functioning, role physical, bodily pain, general health, vitality, social functioning, and role emotional and mental health. Low scores in the eight domains indicate lower quality of life.
Operational Definition of Terms
- Disorders of sexual function was used to characterize difficulties or abnormal sexual functioning.
- Sexual dysfunction was used to refer to a difficulty experienced by one or more individuals during a certain stage of sexual activity involving desire, arousal or orgasm.
- The level of education was evaluated according to the number of years spent in school without repeating class and participants were classified as learned if more than 10 years schooling and not learned if less.
- Anemia was defined as an average of the past four weeks hemoglobin below 9 g/dL.
- The use of erythropoietin was considered effective if the patient received a minimal dose of 8000 IU per month for the past three months.
- Hypertension was considered controlled if the average blood pressure for the last two dialysis sessions was less than 140 mm Hg for the systolic and 90 mm Hg for the diastolic.
Statistical Analyses
Baseline variables are summarized as mean and standard deviation (SD) or median and 25th-75th percentiles for continuous variables. The Pearson chi square test and Mann-Whitney U test were used to compare groups of participants for qualitative variables. Simple Linear regression was used to test for associations between sexual function scores as the outcome variable and various characteristics. A two-tailed P value < 0.05 was considered statistically significant. All analysis were performed using Epi info version 7 software.
III. RESULTS
A total of 52 out of 83 eligible adult women completed the questionnaires, giving a response rate of 63%. Among non-respondents, 25 (30%) refused to take part to the survey, three (3.6%) had no sexual experience before the study, two (2.4%) returned incomplete survey questionnaires and one (1.2%) had uncontrolled heart failure. The mean age of respondents was 38±13 years with range of 18-69, much younger than non-respondents (47 ± 12 years, p= 0.0012). Non-responders were less educated (p<0.0001). The median duration dialysis was 36 (16-60) months. Hypertension and chronic glomerulonephritis constituted 58% of the background nephropathy. Only one patient was diabetic. Anemia defined as hemoglobin level less than 9g/dl was present in 55.8% of the study population and only 27.07% of the patients were currently on erythropoietin. Other characteristic are shown in Table 1.
Demographic and clinical data patients.
| Parameters | Numbers (%) | Means ± SD | Median (IQI) |
|---|---|---|---|
| Demographic data | |||
| Age years | 38.8 ± 13.0 | ||
| Duration in dialysis in months | 36, 16-60 | ||
| Living with a partner | 34 (65.80%) | ||
| House Wife | 12 (23.07%) | ||
| Leaned | 36 (69.00%) | ||
| Post-Menopausal | 18 (34.50%) | ||
| Baseline nephropathy | |||
| Chronic Glomerulonephritis | 20 (38.40%) | ||
| Hypertension related | 10 (19.23%) | ||
| Chronic Interstitial Nephritis | 10 (19.23%) | ||
| Diabetes | 01 (01.90%) | ||
| Unknown | 11 (21.10%) | ||
| Some Clinical data | |||
| Anemia | 29 (55.76%) | ||
| Use of Erythropoietin | 14 (27.00%) | ||
| Uncontrolled HTN | 21 (40.38%) | ||
| Obesity | 12 (23.07%) | ||
| PTH < 300 | 13 (25.00%) | ||
| HCV Positive | 10 (19.23%) | ||
| albuminemia < 30 | 04 (07.60%) | ||
| HVB positive | 02 (03.80%) | ||
1. Prevalence and Type of Abnormalities
Disorders of sexual function were present in all women included in the study (Fig. 1). These disorders were sexual dysfunction (75%), abnormalities of the menstrual cycle (83%) amount women of child bearing age and Sexual inactivity (30%).
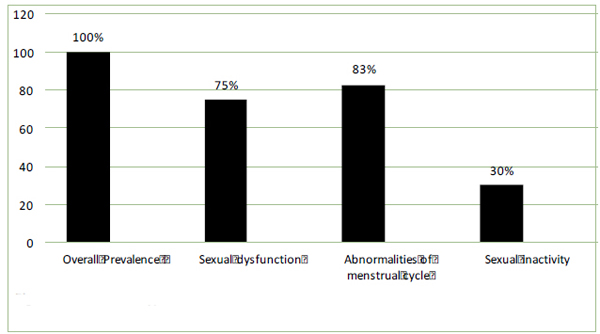
Prevalence and type of abnormalies of sexual function.
2. Description of the Disorders of Sexual Function, Depression and Quality of Life Table 2
All domains of sexual dysfunction were affected. Sexual satisfaction and desire were more affected. In detail, these disorders included: decreased sexual desire (56%), decreased sexual arousal (39%), decreased vaginal lubrication (49%), and failure to achieve orgasm (46%), sexual dissatisfaction (51%), and dyspareunia (36%).
Disorders of menstruations varied in the women of child-bearing age. Irregular menses and non-gravid amenorrhea were more frequent (45% and 40% respectively). Ten women had more than one menstrual disorder.
Depression was present in 5 (10%) patients and was severe in 2 patients. All aspects of the quality of live were affected with social aspect being more implicated and found in 75% of patients.
Prevalence of different aspects of sexual function abnormalities, depression and quality of life.
| N | % | |
|---|---|---|
|
Sexual dysfunction (n= 52) Decrease desire Decrease arousal Decrease lubrication Orgasm failure Sexual dissatisfaction Dyspareunia Global |
28 15 19 18 25 14 39 |
56% 39% 49% 46% 50% 36% 75% |
|
Abnormality of menses (n= 31) Irregular Menses Non gravid amenorrhea Polymenorrhea Oligomenorrhea Metrorragia Menorragia Global |
14 12 08 08 02 01 26 |
45% 40% 25% 25% 6.2% 3.1% 83% |
| Sexual inactivity (n=50) | 15 | 30% |
| Depression | 5 | 10% |
|
Quality of live (n=52) Somatic aspect Social aspect Environmental aspect Psychological aspect Global |
14 39 13 17 17 |
27% 75% 25% 33% 33% |
3. Reproductive Health
Child desire was present in 28(68%) women of child bearing age associated to the marital status (Odds Ratio= 0.1583, 95% I.C. : 0.0649 - 0.3860, P= 0,0002) and inversely proportional to the number of children ((r^2= 0,08 ; Std Error = 0,588 ; P = 0,000967).
Only 7% of women sexually active declared the use of contraceptive method
History of pregnancy was found in 04 (7.84%) women. The pregnancies ended with 03 early spontaneous abortions and one premature delivery.
Only 31% women above 40 declared a Pap smear exam in the past two years.
4. The Clinical Characteristics Associated With Sexual Dysfunction
As shown in Table 3, old age (p=0.0004), diabetes (p=0.0012), marital status (p=0.0045), anemia (p=0.0001) and depression (p=0.0007) had a significant association with the sexual dysfunction. No association was found with education, menstruation position and uncontrolled blood pressure. Social aspect of life quality (p = 0.0391), psychological aspect of life quality (p=0.0323) and total score of quality of live (p=0.0002) had significant association with sexual dysfunction.
DISCUSSIONS
In this study, we found that all women on maintenance hemodialysis presented at least one abnormality of sexual function including sexual dysfunction, abnormalities of menstrual cycle, and sexual inactivity. A myriad of sexual problems affect women with chronic kidney disease (CKD), including decreased libido, dysmenorrheal, and infertility. Hormonal alterations along with vascular, neurologic, psychogenic, and other factors, such as medications, contribute to the development of sexual function abnormalities [8].
Concerning sexual inactivity, Holley et al found a similar prevalence (33%) in America [15]. Arslan and al [16], describing lack of sexual activity reported as frequency of sexual intercourse less than two in the past four weeks in male patients on maintenance hemodialysis found a higher prevalence (78%) in Turkey. The rate is higher when compared to the general population and can be explained by many factors including fragile health condition of people with CKD, hormonal disturbances leading both to organic and psychological variables that can influence the levels of sexual interest in women [15]. Furthermore the persistence of physical asthenia related to the dialysis technics and other comorbidities is the reason advanced by most patients.
Menstrual problems are common among women with ESRD. This is partly because of abnormal bleeding due to platelet dysfunction and also because of failure to ovulate or sustaining adequate corpus luteum function (3).
The frequency of menstruation in women of childbearing age with ESRD is variable, between 8% and 10% [17]. We found a prevalence of 83 % for menstrual abnormalities in the women of child-bearing age. Ghazizadeh et al [18] found the same prevalence in female patients on waiting list for kidney transplant and showed that menstrual problems
Relationship of sexual dysfunction with selected characteristics.
| Parameters | N (%) | P |
| Age | 0.0004 | |
| Duration in dialysis | 0.2831 | |
|
Menstrual status Post-menopausal With menstrual cycle |
12 (67%) 27 (70%) |
0.2029 |
|
Marital Status Living with a partner Not living with a partner |
23 (67%) 16 (88%) |
0.0045 |
|
Education Learned Not learned |
23 (66%) 16 (88%) |
0.0901 |
|
Depression Have Does not have |
4 (80%) 35 (68%) |
0.0007 |
| Anemia | 0.0000 | |
|
Diabetes Have Does not have |
1(100%) 38(74%) |
0.0012 |
|
hypertension Controlled Non controlled |
27 (70%) 21 (40%) |
0.0738 |
|
Poor Quality of live Global Yes No Somatic aspect Yes No Environmental aspect Yes No Psychological aspect Yes No Social aspect Yes No |
17 (89%) 22 (56%) 14 (65%) 25 (70%) 13 (54%) 26 (58%) 17 (90%) 22 (62%) 39 (100%) 0 (00%) |
0.0002 0.2001 0.3802 0.0324 0.0396 |
persisted after kidney transplantation in up to 51% of patients. The mean age of menopause in our study was 36±7 years. Women with CKD tend to experience premature menopause, on average 4.5 years ahead of their healthy counterparts [19] and changes in hypothalamic-pituitary function are the main suggested reasons. Irregular menses, non-gravid amenorrhea were the main abnormalities observed in this study. Perez and al reported that women with end-stage renal disease (ESRD) are usually amenorrheic or had irregular menstrual cycles [20]. Ghazizadeh et al [21] pointed the polymenorhea frequently found in this group of patient as a considerable cause of anemia leading to blood transfusion.
In the present study, 75% of women undergoing hemodialysis had a total score of sexual function less than 28. All domains of sexual dysfunction were affected. Asadifard et al [22] found a prevalence of 100% in 100 Irish women undergoing maintenance hemodialysis with almost the same distribution in different domains and using the same cutting point. In Seethala’s study, 80% of women undergoing hemodialysis had a score of sexual function index less than 26.55 (7). More recently, in a large multicentric cross-sectional study, Strippoli et al [11] reported that 84% of women on maintenance hemodialysis had sexual dysfunction based on a cut-point of 26.55. The prevalence of sexual dysfunction in women who are of an age similar to that of our cohort and who have normal kidney function remains incompletely investigated. Probably, disorders in ovary function and changing in sexual hormones level, psychological problems vascular and neurological disorders, suffering from chronic illnesses and drugs side effects contribute to sexual problems of women on maintenance hemodialysis. The prevalence of sexual dysfunction in women undergoing hemodialysis in this study was a less than other studies. The observed difference can be attributed to differences in study type, sampling, sample size, age differences, entry criteria to study and socio-cultural factors.
Advanced age and diabetes had significant associations with sexual dysfunction. The association of increasing age with sexual dysfunction has been previously demonstrated in nonuremic subjects [23]. Strippoli’s study showed that the prevalence of sexual dysfunction increased by 8% per 1-year increase [11]. Basok’s study showed that low sexual function had relationship with existing diabetes [12]. Diabetes has negative effect on women sexual function via neurological, vascular, hormonal, and psychosocial disorders [24]. Diabetic neuropathy affects stimuli transfer and sexual response and depression resulting from diabetes causes confidence reduction in her.
In this study, not living with a partner, anemia and depression were inversely associated with sexual dysfunction. Strippolli reported that having a partner correlated with a lower risk of sexual dysfunction, whereas depressive symptoms correlated with an approximately two- to four-fold increased risk for sexual dysfunction. This study was in line with Resic’s study which showed that Erythropoietin injection with increasing hemoglobin’s level improved sexual function of women receiving hemodialysis [25] It is also known that erythropoietin therapy helps improving anemia and improving life quality, fatigue reduction, somatic signs, activity tolerance, life satisfaction, and sexual function [26].
In the present study there was a relationship between life quality score and sexual dysfunction in women undergoing hemodialysis. This finding corroborates Lew-starowicz’s findings showing that women who are undergoing hemodialysis and have lower sexual function index also have lower quality of live [27 ] a finding recently confirmed by Peng and al [28]. It seems that a part of somatic, mental and social health of women is related to their sexual function and marriage relations.
Our study has some limitations. The response rate, though higher than many similar studies, was still low (62%). Research on sexual activity is generally characterized by a bias due to volunteer participation [21]. Women who decline participation tend to have a higher degree of conservatism in sexual attitudes. The sample size was small and the cut-point used to define sexual dysfunction was that of European societies, and could be less appropriate for our population. Studies have shown that the good quality of dialysis positively influenced the sexual functions [28] and having only two sessions of dialysis may have overestimated the prevalence in our population. We couldn’t correlate the dysfunction with the quality of dialysis. The lack of a control group is another major limitation.
CONCLUSION
Sexual function is highly impaired in the female hemodialysis population in this setting. Sexual dysfunction, menstrual abnormalities and lack of sexual activities are the main abnormalities. Sexual dysfunction is significantly associated with increasing age, anemia, diabetes and depression. Subjects with sexual dysfunction have poorer quality of life. The diagnosis and treatment of sexual dysfunction should be included in clinical assessment of female patient on maintenance hemodialysis. Studies with a large sample and diverse population of patients across the continuum of estimated kidney function are needed to refine our findings.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

