All published articles of this journal are available on ScienceDirect.

Laparoscopic Nephroureterectomy: Oncologic Outcomes
Abstract
Purpose of Review:
Laparoscopic radical nephroureterectomy (LNU) is being increasingly performed at several centers across the world. This review analyzes the published perioperative and oncologic outcomes of this procedure.
Recent Findings:
Laparoscopic radical nephroureterectomy (LNU) for upper tract TCC is performed pure laparoscopically (LNU) or hand-assisted (HALNU). The most debated issues for oncologic outcomes are management of the distal ureter and lymphadenectomy. LNU appears to have superior perioperative outcomes when compared to open surgery. Although long-term outcomes after LNU are limited, intermediate term oncologic outcomes are comparable to open nephroureterectomy (ONU), the reference standard.
Summary:
Intermediate term oncologic outcomes for LNU compare well with ONU. Initial long-term oncologic outcomes are encouraging. Prospective randomized comparison between LNU and open surgery is needed to define the role of these modalities in the current context.
INTRODUCTION
Upper tract TCC is relatively uncommon accounting for only 5% of all urothelial tumors [1]. It usually occurs between 6th and 7th decades of life. Classical management consists of open radical nephroureterectomy (ONU), which usually requires one large or two separate abdominal incisions. Since LNU was first reported by the Washington University Group in 1991 [2], the benefits of this procedure regarding perioperative morbidity, cosmesis and convalescence have been established [3-5]. Mainly, there are 2 laparoscopic approaches: pure laparoscopic nephroureterectomy (LNU) and hand-assisted nephroureterectomy (HALNU). Despite the perioperative advantages, some oncological issues remain unclear, mainly management of the distal ureter and the role of lymphadenectomy.
MANAGEMENT OF DISTAL URETER
The management of the distal ureter is still controversial. In 1952, McDonald et al. first reported an endoscopic method to handle the distal ureter [6]. In the laparoscopic era, many attempts have been made to avoid the open approach to the distal ureter, which is still commonly used. Matin et al. (2004) compared the outcomes (median follow-up 23 months) using the two different techniques of en bloc excision of bladder cuff: 36 patients underwent needlescopic percutaneous transvesical cystoscopic secured detachment [7] and 12 underwent laparoscopic extravesical stapling. The stapling technique was associated with a decreased overall survival, decreased recurrence free survival and higher positive surgical margin rate. Kurzer et al. (2006) evaluated 49 patients on a mean follow-up of 10.6 months) and reported
their results after cystoscopic circumferential excision of the distal ureter without primary closure of the bladder cuff with simultaneous ureteral ligation during HALNU [8]. No cases of local pelvic or peritoneal recurrences were reported. Vardi et al. (2006) reported a new technique to manage the distal ureter [9]. They purposed an en bloc excision of the bladder cuff and justavesical ureter during HALNU using a flexible cystoscope and a 5F electrode without repositioning the patient. Mean follow up was 31 months (range 5-44) and none of the 6 patients presented with local recurrence. Recently, Nanigian et al. (2006) reported using robotic assistance in an attempt to decrease the technical challenge of excision of distal ureter in 11 patients [10]. As part of the procedure, they filled the bladder with a saline solution before opening it and aspirated all the fluid to avoid dissemination of cancer cells. In addition to the disadvantage of increased cost, the 6 months follow-up is not enough to evaluate local recurrence.
Since most studies do not show any difference between different methods of handling the distal ureter, the best option is to follow individual surgeon’s preference as long as the fundamental oncological concepts are preserved: having a complete resection of the distal ureter with bladder cuff and avoiding tumor spillage.
LYMPHADENECTOMY
Recently, the importance of extended lymph node dissection for bladder cancer regarding staging and prognosis has been established. Given the histological similarity between bladder cancer and upper tract TCC, lymphadenectomy should also be important for the management of upper tract TCC. Kondo et al. (2007) evaluated 169 patients that underwent open nephroureterectomy divided in 3 different groups: complete lymphadenectomy, incomplete lymphadenectomy and no lymphadenectomy [11]. Extended lymphadenectomy improved survival in patients with pT3 stage or higher. On multivariate analysis, complete lymphadenectomy, T stage and grade were significant prognostic factors for cancer-specific survival. Brausi et al. (2007) reported retroperitoneal lymph node dissection and T stage as the only independent significant prognostic factors on overall survival [12]. Busby et al. (2006) found no difference between ONU and LNU concerning number of lymph nodes retrieved, median number of positive nodes retrieved and median density of positive nodes, showing that lymphadenectomy can be performed in the laparoscopic approach as adequately as in open approach [13].
ONCOLOGICAL OUTCOMES AFTER LNU
Laparoscopic nephroureterectomy is performed utilizing the same surgical principles as laparoscopic radical nephrectomy. A transperitoneal (Fig. 1) or retroperitoneal approach (Fig. 2) can be used. Most surgeons are familiar with the transperitoneal approach, which has the advantage of allowing dissection of the ureter all the way to the bladder. This is essential if endoscopic management of the distal ureter (as previously described) is planned. Surgeons familiar with the retroperitoneal approach to radical nephrectomy can perform the renal part of the operation retroperitoneally, although access to the distal ureter is difficult with this approach. This is best suited to cases where the distal ureter will be managed through an open approach. In either case the ureter is not divided and left in continuity. A clip placed on the ureter will minimize the risk of tumor seeding resulting from manipulation of the kidney. In cases of ureteric tumors, careful attention to wide dissection of the ureter is essential to avoid a positive margin or entry into the ureter with tumor spillage.
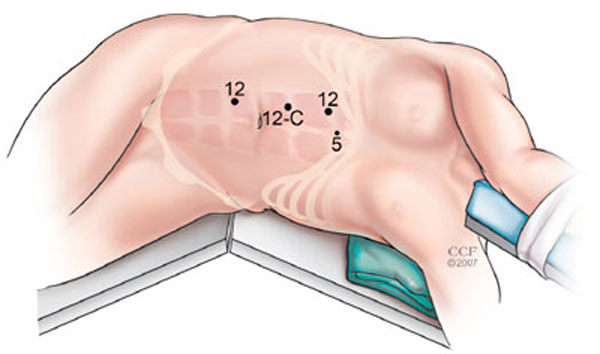
Port placement during right transperitoneal radical nephroureterectomy. (A) primary 12 mm port is placed in the right border of the rectus muscle 3 fingerbreadths above the umbilicus. (B) 12 mm port is placed in the same line 3 cm above the first one (C) 12 mm port is placed in the same line 3 fingerbreadths below the umbilicus. (D) 5 mm is placed in the midline at the sternal angle (and used to retract the liver).
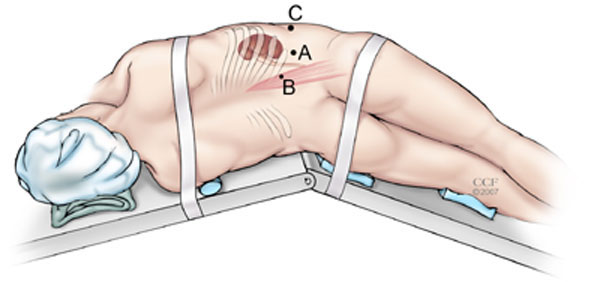
Port placement during right retroperitoneal radical nephroureterectomy. (A) primary 10-mm port is placed at the tip of 12th rib. (B) 10-/12-mm port is placed at junction of lateral border of the erector spinae muscle with lower edge of 12th rib. (C) 10-/12-mm port is placed three fingerbreadths cephalad to iliac crest, between mid and anterior axillary lines.
Long-term follow-up after ONU is well documented in some large series. Charbit et al. (1991) reported the first big follow up series with upper tract TCC in 108 patients [14]. Survival rates after 5 and 10 years were 67% and 65%, respectively. Hall et al. (1998) reviewed 252 patients after ONU (median follow-up 64 months). Recurrence occurred in 67 (27%) patients and urothelial recurrences represented 69% of total [15]. Median time to recurrence was 12 months. Actuarial 5-year cancer-specific survival rates by primary tumor stage were 100% for Ta/Cis, 92% for T1, 73% for T2, and 41% for T3. Median survival for pT4 patients was 6 months. On multivariate analysis, tumor stage was a significant predictor for recurrence, whereas patient age and stage were significant predictors for survival. In contrast, a multicenter study by Ozsahin et al. (1999) evaluated 126 patients with upper tract TCC (median follow-up 39 months) and reported poor oncological outcomes of ONU [16]. In a median period of 9 months, 66% of the patients recurred. The 5- and 10-year overall survivals were 29% and 19%, respectively. Multivariate analysis revealed that independent prognostic factors influencing outcome were T staging, positive surgical margin and tumor in the ureter. Lower survival rates in this study may be explained by high proportions of high grade (76%), non-organ confined disease (59%), and positive surgical margin (26%).
Long term follow-up studies after LNU are still sparse. El Fettouh et al. (2002) reported the results of 116 patients who underwent LNU on a multicenter basis with a median follow-up of 25 months [17]. Positive margins were identified in 4.5% of patients, local recurrence in 1.7%, bladder recurrence in 24% and mean time to recurrence was 13.9 months. Distant metastasis rate was 9%; mean time to metastasis was 13 months. Two-year cancer-specific survival was 87%. According to T stage, 2-year cancer specific survival was 89% for pT1, 86% for pT2, 77% for pT3 and 0% for pT4. Muntener et al. (2007) reported the outcomes of 39 patients after LNU (median follow-up 74 months). Five-year cancer specific survival was 68%. Tumor stage was the only factor related to cancer death and ureteral tumor was the only factor associated with recurrence [18].
Cohorts comparing perioperative and short/intermediate oncological outcomes between ONU and LNU have been published. Bariol et al. (2004) evaluated 25 patients who underwent LNU and 42 who underwent ONU for TCC in a median follow-up of 101 and 96 months, respectively [19]. Local and bladder recurrence rates were 28% (7 patients) for LNU and 42% (15 patients) for ONU while more ureteral tumors were described in ONU. One and 5-year metastases-free survivals were 80% and 72% for LNU and 87% and 82% (table. 1)
LNU Series and Comparative Studies
| Patients (n) | Median Follow-Up (mo) | Recurrence (%) |
Local Recurrence (%) |
Bladder Recurrence (%) | Distant Metas-tasis (%) | Overall Survival (%) |
CancerSpecific Survival (%) |
Risk Factor Associated to Survival (%) | |
|---|---|---|---|---|---|---|---|---|---|
| LNU X Series | |||||||||
| El Fettouh (2002) [17] | 116 | 25 | Not stated | Not stated | 24 | 9 | Not stated | 87 (2 year) | Not stated |
| Muntener (2007) [18] | 39 | 74 | 46 | 5 | Not stated | 18 | 59 (5 year) | 68 (5 year) | Tumor stage |
| LNU X Open Surgery | |||||||||
| Bariol (2004) [19] |
58 26/22 |
101/96 | Not stated | 8/15 | 28/42 | 28/18 | 56/9 | 72/82 (5 year) | Not stated |
| Roupret (2006) [20] |
46 20/26 |
68/78 | 19 (urothelial) | Not stated | Not stated | 10/35 | Not stated | 90/61 (5 year) | Tumor stage and grade |
| Manabe (2007) [22] |
224 58/166 |
14/28 (mean) | 33/38 | 1 case port/2 cases | Not stated | 17/20 | 84/84 (2 year) | 85/82 (2 year) | Tumor stage and grade |
Some recent series report results after hand-assisted LNU (HALNU), but oncologic outcomes are limited. Wolf et al. (2005) evaluated 54 patients who underwent HALNU with median follow up of 25 months [23]. Urothelial recurrences occurred in 66% patients. History of bladder tumors was associated with urothelial recurrence. Non-urothelial recurrences were found in 25% of the patients at a mean 10.4 months follow-up. Age and grade correlated with non-urothelial recurrence. The 2 and 3-year- cancer-specific survival were 86% and 80%, respectively. Organ- confined disease and non organ-confined disease were associated with a 3-year survival of 100% and 36% respectively. High-grade disease correlated with poorer 3-year cancer-specific survival. Chung et al. (2007) also described comparable recurrence free, 3-year cancer-specific and overall survivals in 39 patients after HALNU (median follow-up 48 months) and 41 patients after ONU (median follow-up 62 months) [24].
The propensity for dissemination of high grade TCC is well known. An important concern with laparoscopic approach is port site metastasis. Seven cases have been published so far. No surgical bag was used in six cases and the surgical bag was torn during retrieval of the specimen in one case [24].
Intermediate oncological outcomes after LNU are similar to ONU. Series combining long follow up and large number of patients are lacking. Finally, to confirm these previous encouraging findings, prospective randomized trials are still needed.
CONCLUSION
LNU is now being performed in many centers worldwide. Many series have demonstrated technical feasibility and safety. Although large numbers of 5-year oncologic data are not yet available in the LNU literature, reports indicate that intermediate and long term oncological outcomes are similar to ORC. Carefully designed prospective randomized trials comparing LNU and ONU are necessary to define the role of these modalities in the current and future management of upper tract TCC.

