All published articles of this journal are available on ScienceDirect.

Double Whammy: Pigment Nephropathy and Warfarin-related Nephropathy As Aetiology for Acute Kidney Injury in a Patient With Mechanical Heart Valves
Authors Info & Affiliations
Abstract
It is well known that patients with mechanical heart valves may develop sheer stress related hemolysis and consequent pigment related nephropathy. Warfarin Related Nephropathy (WRN) is a relatively new entity and defined as Acute Kidney Injury (AKI) in the setting of an INR of > 3.0 excluding other obvious etiologies. A biopsy diagnosis of WRN is conducted when red blood cell casts are noted filling and blocking the tubules; additionally, glomerular hemorrhage may be observed. We describe a patient with mechanical heart valves on oral anticoagulation who developed both pigment nephropathy and WRN causing AKI.
1. INTRODUCTION
Warfarin Related Nephropathy (WRN) is a relatively new entity and defined as AKI in the setting of an INR of > 3.0, excluding other obvious etiologies. WRN was first described by Brodsky et al. [1], in 2009 while describing 9 biopsy-proven cases of AKI by distal tubular obstruction with RBCs and proposed the term ‘warfarin-related nephropathy’. It now appears that the newer Direct Oral Anti-Coagulants (DOACs) may also cause a similar clinical and histopathological picture and hence the term Anti-coagulation Related Nephropathy (ARN) has been suggested.
Heme pigment-containing proteins- myoglobin and hemoglobin can cause pigment nephropathy (AKI). Myoglobin is released from muscle in patients with rhabdomyolysis; hemoglobin is released from hemolyzed red blood cells. Renal deposits of iron, hemosiderosis, have been observed in a number of diseases featuring intravascular hemolysis [2]. It is well known that patients with mechanical heart valves may develop shear stress related hemolysis and consequent pigment related nephropathy (AKI) [3].
We describe a patient with mechanical heart valves on oral anticoagulation (warfarin) who developedboth pigment nephropathy and WRN causing >AKI.
2. CASE REPORT
33 year old male, known Hypothyroid (diagnosed 4 years ago) on thyroxine supplementation, Bipolar disorder on Tab sodium valproate and rheumatic heart disease with Mitral Valve and Aortic valve Replacement 8 years previously, on anticoagulation (warfarin) therapy came to the OPD with complaints of abdominal pain, nausea and decreased urine output since 2 weeks. The patient had an episode of acute gastroenteritis 2 weeks prior to these symptoms.
In the past, he had been diagnosed to have severe aortic stenosis with moderate aortic regurgitation, severe mitral stenosis with moderate mitral regurgitation, moderate pulmonary artery hypertension and a left atrial(LA) clot. He underwent double valve replacement surgery in 2010.AV replacement with St. Jude Aortic valve prosthesis (size 19mm) and MV replacement with St. Jude Mitral valve prosthesis (size 23mm) had been performed along with LA clot removal. He had been started on warfarin thereafter. Prior to admission, he was on 3mg of warfarin per day. An INR of 2.8 was noted 2 months earlier.
The examination revealed a Blood Pressure of 110/70 mm of hg with a pulse rate of 160 beats per minute, an irregularly irregular pulse, with prosthetic valve heart sounds well heard. He had subcutaneous ecchymoses on the right forearm and left arm.
Investigations showed an elevated serum creatinine of 4.37mg/dl, Urea 97mg/dl, Hb 11gm/dl, TC 9500/µl, platelet count 190000/ µl. The urine examination revealed plenty of RBCs, 1+ albuminuria. There was no macrohematuria at the time of presentation or later during the course of the illness. 24 hour urine protein collection was 1.56gm/day. Complements C3 and C4 were normal. The Thyroid Function Tests were within normal limits. The ultrasound examination of the abdomen showed RK 10.9cm, LK 11.4 cm with increased cortical echotexture, normal urinary bladder, and normal Liver and Spleen. Prothrombin Time was prolonged, INR was 4.57. Peripheral smear showed hemolysis with schistocytes, Reticulocyte count was 2.3%, and the Lactate Dehydrogenase (LDH) was 1003 units/L, Coomb’s test was negative, Haptoglobin level was low at 20mg/dl. Echocardiography revealed unremarkable mitral and aortic valve prosthesis, Left Ventricular Hypertrophy with variable function due to rapid ventricular rate, and an ejection fraction of 72%. Warfarin was withheld and the Coagulation profile was corrected with Fresh Frozen Plasma and vitamin K, and the patient underwent a renal biopsy on Day 3. Four hours after the biopsy, he developed dyspnea with Atrial Fibrillation and rapid ventricular rate, requiring ICU care and IV amiodarone.
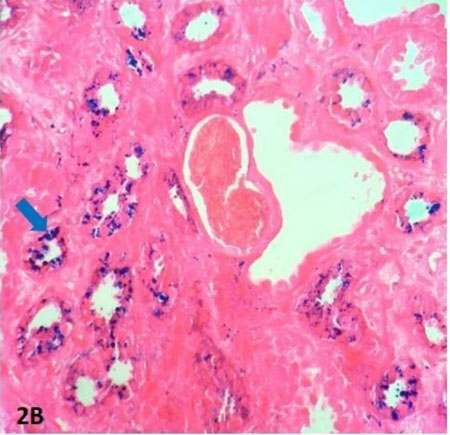
The biopsy showed tubules with moderate degree of Acute Tubular Necrosis (ATN), the distal tubular lumina were blocked with fresh RBC casts at many places, lacking iron pigment (Fig. (1A) and Fig. (1B). Numerous coarse brownish pigments were also observed in the cytoplasm of the proximal tubular epithelium. Additionally, these pigments stained blue with prussian blue stain indicating the presence of heme content. (Fig. (2A) and Fig. (2B) These findings confirmed the presence of warfarin related nephropathy and pigment nephropathy. Immunofluorescence showed mild IgA deposition in the mesangium (1+), and no c3, IgG, c1q deposits. Electron Microscopy was not performed.


The patient was treated with Low Molecular Weight Heparin and IV Fluids for the next 4 days. There was a gradual decrease in the serum creatinine and at discharge, it was 2.2 mg/dl. The patient was started on dabigatran but this was quickly switched back to warfarin based on literature findings that the DOAC was contra-indicated in the context of mechanical heart valves. On further out-patient follow up after a week, the serum creatinine settled to normal (1.02mg/dl). He was on 3mg of Warfarin per day and the INR was 2.3. A repeat urine examination at follow up showed RBCs 0 to 1 and no albuminuria.
3. DISCUSSION
This patient with mechanical (St Jude) heart valves (Mitral and Aortic) on oral anticoagulation, warfarin, presented with AKI and a renal biopsy showed the presence of both pigment nephropathy and Warfarin Related Nephropathy.
Hemolysis is seen more commonly with mechanical heart valves than bioprosthetic valves. In one series, hemolysis was noted to occur in 51.2 percent in patients with St. Jude valves and 17.8 percent in patients with Medtronic Hall valves [4], but the hemolysis was usually mild and subclinical, reflected by mild elevations in the serum LDH levels. The heme pigment that is released during hemolysis is filtered by the Glomerulus and is toxic to the kidney, causing pigment nephropathy.
Three mechanisms have been described whereby heme pigment may cause renal damage - tubular obstruction, direct proximal tubular epithelial cell injury and vasoconstriction, which results in a reduction in blood flow in the outer medulla. Despite its toxic properties, heme pigment rarely causes kidney injury in the absence of predisposing conditions, which include volume depletion, metabolic acidosis, and, possibly, mild ischemia. In our patient, the occurrence of diarrhea in the recent past is significant in that it contributed to dehydration and this, together with the obstruction of the renal tubules by red blood cell casts and direct tubular toxicity by the hemoglobin released from the hemolysis of the extravasated red blood cells, contributed to worsening kidney dysfunction.
The other clinical state where pigment nephropathy occurs is rhabdomyolysis. Medullary vasoconstriction and intra-renal hypoxia may play a role in myoglobin-induced renal failure. The deterioration in kidney function appears to reflect the combined effects of cortical damage, medullary hypoxic injury, and tubular obstruction [4, 5].
WRN is defined as AKI in the setting of an INR of > 3.0, after excluding other obvious etiologies. In 2009, Brodsky et al. were the first to describe this entity and presented a case series of nine patients of unexplained AKI associated with supra-therapeutic INRs in patients on warfarin. Kidney biopsy was performed in every patient and revealed acute tubular injury, glomerular hemorrhage and renal tubular obstruction by RBC cast [1]. Brodsky et al. again undertook a retrospective analysis of the records of 15,258 patients who were started on warfarin therapy between January 2005 and 2008 at the Ohio State University Medical Centre. WRN occurred in 20.5% of the entire cohort, 33.0% of the Chronic Kidney Disease (CKD) cohort, and 16.5% of the non-CKD cohort. One-year mortality was 31.1% in patients with WRN versus 18.9% in patients without [6].
Recent evidence suggests that WRN-like syndromes are not confined to anticoagulation with warfarin, but may be seen with other anticoagulants, such as dabigatran. In a study on rats, Dabigatran resulted in changes in coagulation in rats similar to those in humans at 50 mg/kg/day. Dabigatran resulted in a dose-dependent increase in serum creatinine (Scr) and hematuria in both control and 5/6 nephrectomy rats. Morphologically, numerous RBC tubular casts were seen in 5/6 nephrectomy rats [7, 8]. Therefore, the term “anticoagulant-related nephropathy” has been proposed because the entity has been associated with anticoagulants other than warfarin.
The decision to do a renal biopsy in the scenario of an anti-coagulated patient is tricky and fraught with risks. The possibility of a bleed after the biopsy is foremost in the mind of the nephrologist while the withdrawal of anti-coagulation leading to unwanted clots on the flip side is worrying. So much so, biopsies are deferred in such clinical situations and as a result, a rare diagnosis is missed.
The plan of switching our patient to Direct Oral Anti-Coagulation (DOAC) was discussed with the cardiologist and the use of dabigatran or apixaban was considered. But a literature review showed that DOACs should not be used in patients with mechanical prosthetic heart valves. All patients with mechanical prosthetic valves require lifelong Vitamin K Antagonist (e.g, warfarin) anti-coagulation. This was based on the results of the RE-ALIGN trial, which showed no benefit and an excess of thromboembolic and bleeding risk with dabigatran as compared with warfarin [8]. In RE-ALIGN, patients who had undergone mechanical valve replacement were randomly assigned to receive either dabigatran or warfarin; the trial was stopped early because of the excess of thromboembolic and bleeding events in the dabigatran group. None of the other DOACs, rivaroxaban, apixaban or edoxaban have been studied in patients with mechanical prosthetic heart valves and are not approved therefore, for use in patients with mechanical heart valves. Therefore, we decided to switch our patient back to warfarin, but counseled the patient and relatives on the need to monitor the INR very closely so that it does not exceed to 3.0.
CONCLUSION
Our patient had histo-pathological features of both pigment nephropathy and Warfarin Related Nephropathy (WRN). The latter finding is a relatively new entity and it would augur well for us not only to be aware of this condition but also to look at AKI in the context of the use of all oral anticoagulation be it warfarin or the DOACs (and in various other clinical scenarios as well) with this new information in mind.
LIST OF ABBREVIATIONS
| WRN | = Warfarin Related Nephropathy |
| AKI | = Acute Kidney Injury |
| DOACs | = Direct Oral Anti-Coagulants |
| ARN | = Anti-coagulation Related Nephropathy LDH= Lactate Dehydrogenase |
| ATN | = Acute Tubular Necrosis |
| CKD | = Chronic Kidney Disease |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Informed consent was obtained from the patient.
STANDARD FOR REPORTING
CARE guidelines and methodology were followed.
CONFLICT OF INTEREST
The authors declare no conflict of interest, financial or otherwise.
ACKNOWLEDGEMENTS
Declared none.

