All published articles of this journal are available on ScienceDirect.

LEARNING FROM IMAGES
61-year-old male patient presented with chief complaints of recurrent right renal colic and hematuria.
A ‘stone protocol’ non contrast CT scan of the abdomen and pelvis was performed, which revealed hyperdense blood in the pelvicalyceal system (Fig. 1A) and blood clots in the bladder (not shown). A contrast enhanced CT scan of the abdomen and pelvis (Fig. 1B) revealed an infiltrative lesion involving the pelvicalyceal system of the right kidney with thrombosis of the right renal vein. Coronal T1 weighted post contrast MRI image (Fig. 2) revealed an infiltrative mass involving the right kidney with notable absence of caliectasis or hydronephrosis. Thrombus involving the right renal vein and the inferior vena cava was seen as a filling defect. The microscopic examination of the surgical specimen revealed clear cell type renal cell cancer, with tumor extending into the right renal vein and its walls. On surgical exploration, tumor invasion of the renal capsule with extension into the perinephric fat but restricted to Gerota’s fascia was seen.
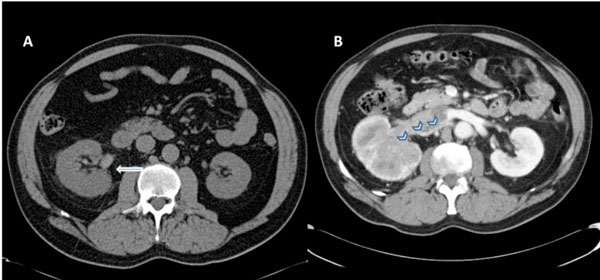
(A) Non-contrast CT scan of abdomen and pelvis demonstrates slightly enlarged right kidney with mild perinephric fat stranding. Note hyperdense blood in the pelvicalyceal system consistent with hematuria (marked by white arrow). (B) Contrast enhanced CT scan of the abdomen and pelvis reveals an infiltrating mass involving the whole kidney with dilated and thrombosed right renal vein (marked by chevrons).

Contrast enhanced fat saturated T1 weighted coronal MRI image demonstrates infiltrative right renal mass with extension of the tumor thrombus into the right renal vein and the inferior vena cava (marked by notched arrow).
Neoplasms account for a significant number of infiltrative renal lesions seen on imaging studies and include a variety of uncommon tumors such as renal medullary carcinoma. However, infiltrative growth is an atypical manifestation (6% of cases) of commonly encountered renal cell carcinoma [1].
The more common subtypes of renal cell cancer -clear cell, papillary, and chromophobe cell-typically appear as well-defined mass and may form a capsule of connective tissue and compressed atrophic renal parenchyma with tumor proliferation. Occasionally, the tumor appears ill-defined and infiltrative; this appearance is more typical of the uncommon sarcomatoid subtype but may be seen with the other subtypes as well.
Absence of caliectasis is usually a clue to the diagnosis of renal cell cancer over transitional cell cancer. However renal vein invasion can occur in both types of carcinoma.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

