All published articles of this journal are available on ScienceDirect.

LEARNING FROM IMAGES: Renal Volume in Polycystic Kidney Disease
INTRODUCTION
Autosomal dominant polycystic kidney disease (ADPKD) is the most common hereditary renal cystic disease. Majority of families with ADPKD have an abnormality on chromosome 16 (PKD1 locus) resulting in end stage renal disease at a mean age of 54.3 years. The diagnosis and management of ADPKD relies primarily on imaging studies. Renal ultrasonography is commonly utilized to screen family members for ADPKD [1]. The ultrasonographic criteria for the diagnosis of ADPKD for at risk individuals are age dependent. Individuals aged 40 -59 years with two cysts in each kidney on ultrasonography is associated with a sensitivity and specificity of 90 and 100% respectively. CT scan (Fig. 1) imaging is more sensitive than ultrasonography and can identify cysts with a diameter of 2-3mm.
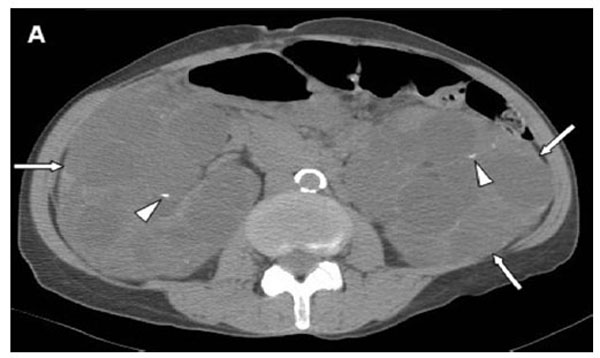
Axial noncontrast CT scan showing enlarged bilateral kidneys (arrows) with multiple cysts of variable sizes. Some of the cysts have partial rim calcifications (arrowheads).
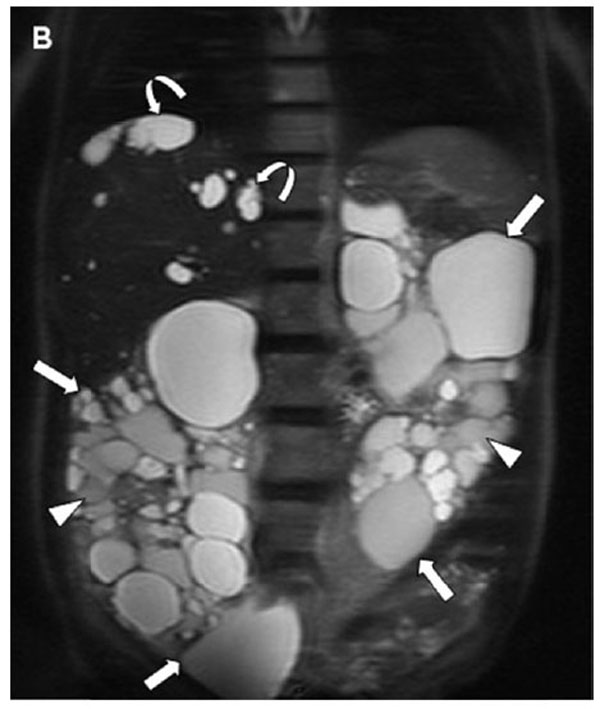
Coronal T2 weighted MRI image showing marked enlargement of both kidneys (arrows) spanning nearly the entire length of abdomen, right kidney is 25 cm in length (volume 1230ml) and left kidney is 24 cm in length (volume 980ml).
Renal function remains intact generally until the fourth decade of life. Some of the risk factors that have been identified for progression of renal disease include: genetic defect (PKD1 vs PKD2), age at presentation, hypertension, male gender, proteinuria, and increased kidney size (larger
kidneys are seen with PKD1). The increasing kidney size and cyst volume has been shown to correlate with worsening renal function. The Consortium for Radiologic Imaging for PKD reported that baseline kidney volume measured by MRI predicted the rate of kidney growth and decline in renal function. Height adjusted kidney volume of greater than 600 ml/m is a better predictor of chronic kidney disease progression over eight years compared to age, proteinuria or baseline serum creatinine [2]. The normal renal volume measured using MRI is 202 ± 36 ml for men and 154± 33 ml for women [3]. The MRI image (Fig. 2) shown here assessed
the right renal volume as 1230 ml and the left renal volume as 980 ml. MRI imaging and renal volume estimation is still considered a research tool but can assist in providing insights into rate of progression of renal disease. Early studies with tolvaptan have shown reduction in total kidney volume with slowing of the decline in renal function over a 3-year period [4].
CONFLICT OF INTEREST
The authors confirm that this article content has no conflicts of interest.
ACKNOWLEDGEMENTS
Declared none.

