All published articles of this journal are available on ScienceDirect.

Cardio Renal Syndromes 2015: Is there a Silver Lining to the Dark Clouds?
Abstract
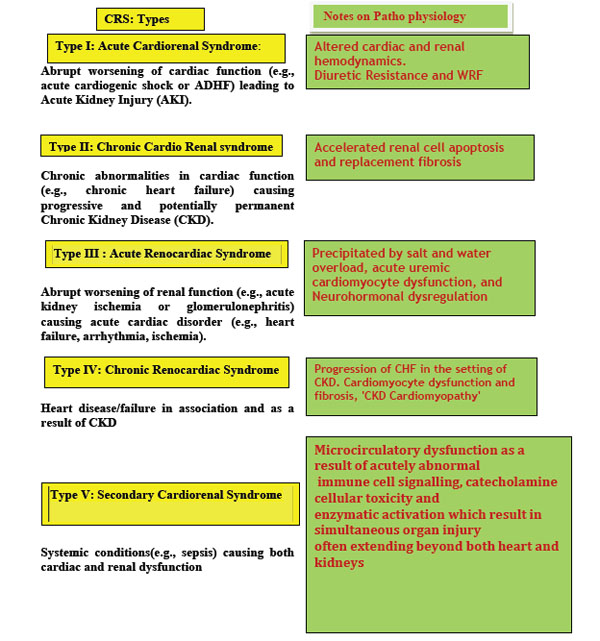
Kidneys have a pivotal role in maintaining our homeostasis. Kidneys and heart work in tandem to maintain volume homeostasis. Heart failure impacts renal function in many ways including renal hypo perfusion but also due to increased venous pressure along with stimulation of various neuro-humoral responses. Renal failure induces cardiac damage and dysfunction by causing volume overload, inflammation and cardiomyocyte fibrosis. Concomitant comorbidities like Hypertension and Diabetes also play important role resulting in Cardiorenal Syndrome (CRS). Acute Dialysis Quality Initiative, 2007 recognized the bidirectional nature and different manifestations of CRS in acute and chronic settings.
Diuretics are the most common drugs to treat the most common symptoms of CRS i.e., peripheral edema and pulmonary congestion. Diuretics could nevertheless contribute to worsening renal function (WRF). Initially it was accepted that WRF during the course of treatment of acute decompensated heart failure (ADHF) uniformly resulted in worse prognosis. However, in view of a few recent studies, the significance of WRF early in response to treatment of ADHF is being debated. The optimal dose and method of delivery of diuretics is still undecided.
Isolated ultrafiltration does not improve renal function in patients with CRS despite the early promise. A large, multicentre trial ruled out any survival benefits with Recombinant Brain Natriuretic Peptide (Nesiritide). Despite good physiological basis and early promise with smaller studies, many drugs like Dobutamine, Rolofylline and Tolvaptan failed to show survival benefit in larger studies. However, two recent studies involving Relaxin and Neprilysin have shown good survival advantage. There had been little progress in treatment of CRS until studies involving Relaxin and Neprilysin inhibitor combination with ARB were published.
There may after all, be a glimmer of hope in the field of CRS bogged by multiple negative studies.
PATHOPHYSIOLOGY OF CRS
Kidneys play a central role in the volume homeostasis of our body. Heart, as the pump contributes towards tissue perfusion and oxygenation. The cross-talk between the kidneys and the heart is important to control blood volume and blood pressure by renal sodium and water excretion. This cross talk occurs via the Low pressure baroreceptor and effector system (consisting of venous and atrial receptors) and the High Pressure System (consisting of arterial and aortic arch receptors with the Juxta glomerular (JG) Apparatus).
Low Pressure System: Atrial-Renal Reflexes
Increase in atrial pressure suppresses release of Arginine Vasopressin through non osmotic stimulus known as Henry-Gauer reflex [1]. As demonstrated in canine experiments, balloon dilatation of left atrium (LA) resulted in diuresis and the same could be abolished by vagotomy. Atrial stretch leads to decreased Adrenocorticotrophic Hormone which in turn causes decreased mineralocorticoid activity. Atrial stretch also results in a reduction of renal sympathetic tone. It also leads to increased release of atrial natriuretic peptide (ANP).
The net result is increased renal salt and water excretion, restoring the intravascular volume and atrial pressure to normalize.
High Pressure System
The arterial and aortic arch baroreceptors with the JG Apparatus constitute the high pressure system. The JG apparatus of the kidney is the key mediator of the activation of the renin-angiotensin aldosterone system (RAAS). Renin also stimulates sympathetic nervous system (SNS).
In Congestive Heart Failure (CHF), the low pressure system responses are attenuated by activation of neuro humoral system caused by arterial under filling leading to salt and water retention. Specifically, renal beta-adrenergic stimulation and decreased sodium chloride delivery to the macula densa stimulate the JG apparatus. Increased Renin secretion with RAAS stimulation and Sympathetic stimulation leads to renal and systemic vasoconstriction. The predominant effect of RAAS on efferent arteriolar constriction leads to increased intraglomerular pressure leading to increased filtration fraction. Thus the blood passing on to Peri tubular capillaries (PTC) will be low in Sodium (Na) leading to enhanced Na reabsorption from the proximal tubule by altering Starling forces in the PTCs [2]. The proximal tubular reabsorption of Na and water is also stimulated by Alpha adrenergic activation.
RAAS also leads to increased expression of Endothelin 1, a powerful vasoconstrictor and potent pro-inflammatory and pro-fibrotic agent in the kidney [3].
Thus, in CHF, activation of the RAAS leads to increasing proximal Na reabsorption and perpetuating volume overload in turn contributing to cardiac dilation and left ventricular hypertrophy. Excessive sympathetic activity can induce myocardial damage, cardiac hypertrophy and focal myocardial necrosis. Increased norepinephrine levels in CHF have been shown to correlate with increased mortality [4]. RAAS causes hyper filtration injury to the glomeruli along with inflammation and fibrosis.
Thus, in CRS, a vicious cycle develops, leading to ongoing structural and functional damage in both organs [5, 6].
Hypertension and Diabetes mellitus are commonly associated with CHF and CRS. The target organ damage due to these conditions in both the kidneys and heart and the resultant interaction between the organ systems also commonly contribute to CRS [7].
Although in CHF the clinical picture is dominated by the action of vasoconstricting and sodium-retaining hormones such as Angiotensin II, Nor Epinephrine, Endothelin, Adenosine, and Arginine Vasopressin [8], there is an attempt by vasodilatory and natriuretic hormones such as Natriuretic peptides, Prostaglandins and Relaxin among others try to offset these deleterious effects (Table 1).
Cardio-renal syndrome: the plethora of neurohormonal activation.
| Cardio-Renal Syndrome: | |
|---|---|
| The Plethora of Neurohormonal activation | |
| Vasoconstrictors | Vasodilators |
| SNS | Natriuretic peptide systems (BNP/ANP) |
| RAAS | Urocortin / Urotensin |
| Vasopressin | Prostaglandins |
| Endothelin | Nitric Oxide |
| Adenosine | Adrenomedulllin |
| Relaxin | |
Major classes of Diuretics used in CRS.
| Generic Name | Class | Initial Dose (mg) | Comments |
|---|---|---|---|
| Furosemide (Frusemide) | Loop | 80 | IV; PO equivalent is~twice the IV dose. Most commonly (ab)used diuretic! |
| Bumetanide | Loop | 0.5 | Oral and IV doses are the same |
| Torsemide | Loop | 5-10 | Best oral availability |
| Ethacrynic acid | Loop | 50 | Used if allergic to furosemide |
| Hydrochlorothiazide | Thiazide | 12.5 | PO; Weak diuretic per se-used with frusemide for sequential tubular blockade of Na reabsorption |
| Metolazone | Thiazide | 2.5 | Only available orally; high risk of hypokalaemia |
Diuretic resistance in ADHF and CRS.
| 1. Failure of diuretics to reach tubular site of action |
| - Decreased G.I. absorption ( Gastro Intestinal edema) |
| - Decreased secretion into tubular lumen (↓ GFR) |
| 2. Compensatory Mechanisms |
| - RAAS, SNS ↑Na reabsorption in PCT |
| 3. Post dose Compensatory retention of Na |
| 4. Tubular adaptation |
| - Chronic Loop diuretic use- RAAS stimulation leading to Hypertrophy and hyperplasia of DCT |
| 5. ↑Aldosterone in CD |
DEFINITIONS OF CRS
The definition of CRS has evolved over the last few years along with greater understanding of the underlying pathophysiology. Since CRS is dominated by pulmonary congestion and edema with WRF, National Heart, Lung and Blood institute initially defined CRS as a state in which treatment to relieve congestive symptoms of heart failure was limited by further decline in renal function. Worsening Renal Function and Diuretic resistance (DR) formed part of definition by Liang et al. [6].
The Acute Dialysis Quality Initiative [7] has broadened the definition of CRS:
- To reflect the broad clinical settings in which CRS occurs and
- To identify different Patho physiology of acute and chronic organ dysfunction.
Many studies including the Framingham Heart Study have underlined the causal relationship between hypertension, diabetes and CHF [9, 10]. These chronic conditions are also the common denominators for the development of CKD. Although ADQI acknowledges the common occurrence of hypertension and diabetes in patients with CRS, currently CRS due to such chronic conditions (with chronic inflammation, fibrosis and damage) is lumped with acute conditions like sepsis in CRS type 5. Hopefully, there will be a revision of CRS classification to reflect the different etiopathologies and different treatment approaches.
Clinical Features of CRS
CRS is most commonly identified in the setting of hospitalization for ADHF. Most patients are volume overloaded with peripheral and pulmonary edema with elevated jugular venous pressure. Some patients may be in severe hypotension and have intravascular volume depletion. There is oliguria and WRF which may be exacerbated with attempts to achieve vigorous diuresis.
Significance of Increased CVP in CRS
WRF has been reported in patients with ADHF despite preserved left ventricular EF.
A study of electronic medical records of 2,557 patients in Netherlands who underwent right heart catheterization for evaluation of various cardiovascular diseases revealed that a CVP measurement of more than 6 mm Hg was significantly associated with decreased eGFR and an independent predictor of reduced survival on multivariate analysis [11].
In another study of 145 consecutive patients admitted with ADHF, elevated CVP correlated with worse outcome even in patients with preserved cardiac pump function [12]. In this study urine albumin excretion was often increased at the time of admission to hospital and decreased significantly within 7 days of treatment. The increase in renal vein pressure as a direct transmission from increased IVC pressure leads to decreased GFR and increased albuminuria.
Importance of Elevated Intra-abdominal Pressure (IAP) in CRS
Normal IAP is between 5-7 mm Hg. Mullens et al. demonstrated that elevated IAP in patients with ADHF is associated with WRF [13]. Elevated IAP of >12 mm Hg recorded by transvesical technique in 40 consecutive patients correlated with WRF. Notably not many of these patients had ascites, suggesting the possibility of increased splanchnic venous pressure contributing to elevated IAP.
ANEMIA IN CRS
Anemia in CRS is multi factorial. Iron deficiency can occur due to occult GI bleeds being on anti-platelet drugs or anti coagulation or angiodysplasia associated with CKD. There may be contribution from hemodilution of CHF. The CKD related Erythropoietin (EPO) underproduction and inflammation related EPO unresponsiveness may all add to the anemia in CRS. In fact Silverberg et al. coined the term Cardiorenal Anemia and advocated for aggressive correction of anemia to reverse the cardiac and renal damage [14].
A study was undertaken in Europe looking at correcting iron deficiency in 459 patients with CHF irrespective of Haemoglobin (Hb) levels. In the FAIR-HF study, patients with iron deficiency were randomized to receive intravenous ferric carboxymaltose or placebo. There was an improvement in symptom score and New York Heart Association (NYHA) functional class in those receiving intravenous iron compared to those receiving placebo, irrespective of the Hb levels. However, in this study, patients with significant renal dysfunction were excluded [15].
While correcting severe anemia and iron deficiency is worthwhile to achieve Hb levels of around 10g/dL, normalization of Hb has not been found to improve outcomes. A large multicentre randomised double blind placebo controlled trial (RED-HF study) of Treatment of Anemia with Darboepoitin Alfa in Systolic Heart Failure in 2278 patients with Hb between 9-12g/dL to achieve a Hb of 13 g/dL did not improve clinical outcomes. The primary outcome was a composite of death from any cause or hospitalization for worsening heart failure [16]. Of note, study patients in this study had mean estimated glomerular filtration rate (eGFR) of around 45ml/min/1.73m2 placing them in CKD stage 3.
PROGNOSIS OF CRS
The survival of patients with stable CHF has improved considerably in the last 2 decades with the use of Angiotensin Converting Enzyme (ACE) inhibitors or Angiotensin Receptor Blockers (ARB), beta-blockers and mineralocorticoid inhibitors. However, the prognosis of patients with ADHF and CRS remains grim with 3- month mortality in excess of 25% in various studies.
Renal function is the single most determinant of survival in patients with CRS.
In a study of a subgroup of 372 patients from the PRIME ii study looking at the correlation between renal function, neurohumoral activation and survival in patients with CHF, impaired renal function was the strongest predictor of mortality. It was a stronger predictor than impaired cardiac function (LVEF and NYHA class) in advanced CHF [8].
In the OPTIMIZE-HF registry report of more than 48,000 patients with ADHF, serum creatinine along with systolic BP, serum sodium and heart rate correlated with mortality [17].
ADHERE, a large data base of nearly 1 million CHF patients in the USA has proposed a practical bedside tool for mortality risk stratification. The three strongest predictors of mortality are:
- BUN > 43 mg/dl (15.5 mmol /l)
- Systolic BP < 115 mmHg
- Serum creatinine > 2.75 mg/ dl (242umol/l) [18].
In a recent study of 186 patients admitted with ADHF, Neutrophil Gelatinase Associated Lipocalin (NGAL), a marker of kidney injury, predicted adverse outcomes at 30 days compared to BNP levels [19].
Although elevated serum creatinine during treatment of ADHF is often taken to represent WRF, the scenario is more complex. Increased serum creatinine during treatment of ADHF may reflect hemoconcentration and thus effective diuresis rather than WRF. On the other hand lower creatinine during treatment may reflect persistent and worsening fluid overload. In fact, Testani et al. demonstrated in 336 patients that elevated serum creatinine as part of hemoconcentration (associated with increases in serum protein and haematocrit) was associated with a better 180 day survival [20].
Because Urea nitrogen absorption at PCT is under the influence of RAAS, BUN has been proposed as a surrogate prognostic marker of neurohumoral activation in ADHF [21]. Elevated Blood Urea nitrogen (BUN) was found to be predictive of mortality at 1 month in a multivariate analysis in 526 patients while serum creatinine, Cystatin C and NT-pro BNP were not predictive [22].
DIURETICS IN CRS
ADHERE analysis revealed that dyspnea and pulmonary congestion on x-ray were the most common features of CRS accounting to 89 and 74 percent on admission respectively. Thus, it is not surprising that diuretics are the commonest drugs used.
The immediate symptomatic beneficial effects of diuretics are brought about by:
- Improved Pulmonary congestion
- Decreased Ventricular Wall stretch and Ventricular dilatation
- Venodilation leading to immediate reduction in preload (with IV Furosemide) [23].
The well documented adverse effects of diuretics are:
- Hypotension
- Hypokalaemia and Hypomagnesaemia causing arrhythmias
- Loop diuretics block Na reabsorption by Macula Densa directly leading to Renin stimulation even in the absence of volume depletion [24]
- Volume depletion leading to further stimulation of RAAS/ SNS [25]
- Worsening Renal Function (WRF).
Table 2 summarizes the major classes of diuretics used in CRS.
The way diuretics should be used to achieve maximum efficacy with minimal side effects has been the topic of much debate. In a recent 2x2 factorial design double blind, randomised study 308 patients with ADHF were assigned to IV infusion or IV bolus dose of furosemide at a low dose or a high dose [26]. There was no significant difference in patient’s global assessment of symptoms or in the mean change in the creatinine levels with bolus injections or continuous infusion. In the comparison of the high-dose (2.5 times previous oral dose) strategy with the low-dose strategy (equal to previous oral dose), again there was no significant difference in patient’s global assessment of symptoms between the groups.
The high-dose strategy was associated with greater diuresis and more favourable outcomes in some secondary measures but also with transient worsening of renal function. As noted earlier, the importance of this WRF in the setting of diuretic use is a topic of debate. Given the greater diuresis and continuous action, high dose continuous Furosemide infusion has been the author’s personal preference.
DIURETIC RESISTANCE
Inability to get rid of edema despite liberal diuretic use is called diuretic resistance. Epstein et al. defined diuretic resistance as failure to excrete at least 90 mmol of sodium within 72 hours of a 160 mg oral furosemide dose given twice daily [27].
The mechanisms of DR are summarised in Table 3.
Diuretic Resistance is a major feature of admissions with ADHF and CRS. In the ADHERE analysis requirement of IV Furosemide of more than 160mg/day was associated with increases in In-hospital mortality, Length of stay and Worsening Renal Function (WRF).
Combining the diuretics so that there is sequential tubular blockade of Na and water reabsorption is a logical step often undertaken by combining loop and thiazide diuretics [27]. Although Aldosterone receptor antagonist Spironolactone has been shown to reduce myocardial fibrosis and improve survival in patients with heart failure [28], its use is often limited by hyperkalemia in CRS.
ULTRAFILTRATION IN CRS
Isolated ultrafiltration (UF) achieved by peripheral vein catheterization using Aquadex Flex Flow machine allows slow UF rates (10-40ml/min) and requires low extra corporeal blood volumes of 33-40 ml. Thus it was thought unlikely to upset the hemodynamic stability or stimulate SNS and RAAS. After several smaller studies suggested that isolated UF in patients with ADHF may lead to better outcomes compared to diuretics, UNLOAD study was undertaken [29]. 200 patients hospitalized for ADHF were randomized to UF or intravenous diuretics. Primary end points were weight loss and dyspnea assessment at 48 h after randomization. Secondary end points included net fluid loss at 48 h, functional capacity, CHF rehospitalisation and unscheduled visits within 90 days. Safety end points included changes in renal function, electrolytes, and blood pressure. Ultrafiltration produced greater weight and fluid loss than intravenous diuretics and resulted in significant reductions in the rate and length of rehospitalisation and unscheduled medical visits for ADHF. One important exclusion criteria was moderate-advanced renal dysfunction as defined by a serum creatinine of more than 3mg/dl (264 umol/l). However, the mortality rates did not differ in the 2 groups. Nine deathsoccurred in the ultrafiltration group and 11 in the diureticsgroup over the 90 day study period.
A randomised trial was performed to establish the success with UF in CRS with more severe renal dysfunction but failed to achieve benefits. CARESS-HF trial was a
randomised trial in 188 patients with CRS comparing stepped pharmacologic treatment with ultrafiltration. Patients with serum creatinine up to 3.5 mg/dl (309.4umol/L) were enrolled. UF rate was 200 ml/hour. The primary end point was the bivariate change from baseline serum creatinine and body weight at 96 hours. Unfortunately, those who received UF showed worsening of creatinine and similar weight loss associated with higher incidence of serious adverse events (72% vs 57%) [30]. The study generated extensive discussion regarding optimal rates of UF as well as the significance of WRF in this setting. The exhaustive diuretic strategy employed for the diuretic arm of the study is unusual in daily clinical practice.
UF may have a role early in ADHF rather than when severe renal dysfunction has set in.
BNP TRIALS IN CRS
B-type natriuretic peptide (BNP) provides beneficial effects physiologically by counteracting many of the maladaptations in CHF. It inhibits the vasoconstriction caused by RAAS and Endothelin-1 and other vasoconstrictors. BNP enhances sodium excretion and promotes diuresis. Thus lot of hope was pinned on BNP in treatment of ADHF. FDA licensed the use of Nesiritide, a recombinant BNP in 2001 for use in patients with ADHF on the basis of small studies showing a reduction in pulmonary-capillary wedge pressure and improvement in dyspnea at 3 hours. However, in a large multi-centre, placebo controlled study involving 7141 patients across 398 centres, Nesiritide did not decrease the rate of death and rehospitalisation and had a small, non-significant effect on dyspnea when used in combination with other therapies. Nesiritide was not associated with a worsening of renal function, but it was associated with an increase in rates of hypotension. On the basis of these results, the authors concluded that Nesiritide could not be recommended for routine use in the broad population of patients with ADHF [31].
OTHER NEGATIVE TRIALS IN CRS
Tolvaptan (EVEREST Trial): Vasopressin mediates fluid retention in CHF. Tolvaptan, a vasopressin V2 receptor blocker, was studied in patients with symptomatic HF. Tolvaptan initiation within 48 hours of hospitalization with long-term continuation of therapy, resulted in neither improvement nor reduction in survival nor in the combined end point of cardiovascular mortality or HF hospitalization [32].
PROTECT study: In CHF, increased levels of Adenosine are secreted by the JG apparatus. Adenosine acts via Adenosine A1 receptors to cause afferent arteriolar constriction and increased Na absorption in the Proximal Convoluted Tubule contributing to worsening renal function (WRF) and Diuretic Resistance (DR). The pilot study had shown efficacy of Rolofylline, an Adenosine A1 receptor antagonist, in relieving symptoms of dyspnea with less worsening of renal function. However, PROTECT study in which 2033 patients with ADHF and CRS were randomly assigned in 2: 1 ratio to Rolofylline or placebo failed to demonstrate any benefit in the treatment arm with regard to renal function or rehospitalisation or death [33]. There was a higher incidence of neurological complications with Rolofylline.
The Renal Optimization Strategies Evaluation (ROSE) trial was a recent clinical trial conducted by the National Institutes of Health, National Heart, Lung and Blood Institute (NHLBI) Heart Failure Clinical Research Network. In this trial, 360 participants with ADHF and CKD were randomly assigned to 3 groups: one third to standard diuretic-based decongestive therapy, one-third were given low-dose dopamine (2mcg/kg/min infusion) in addition to standard therapy, whereas another third received low-dose Nesiritide (0.005-mg/kg/min infusion for 72 hours) in addition to standard anti-failure therapy. Primary end points were total cumulative urine volume and change in serum Cystatin C. There were no statistically significant differences in UOP, Cystatin C levels, rehospitalisation or death at 60 days which remained high at 25% [34].
After many negative studies despite a sound physiologic basis, finally some recent trials have shown promise of improved symptom control and survival in CRS.
RELAXIN
Relaxin is a well-known human reproductive hormone. It is a peptide hormone produced by corpus luteum, endometrium, placenta and breast in females. Relaxin is also produced in males by the prostate and heart. Serum Relaxin levels are identical in males and females. Receptors for Relaxin are found in brain, kidney, heart, uterus, testis and placenta. It causes muscle relaxation and vasodilatation by increasing cyclic AMP. It also has antifibrotic property by decreasing TGF-B pertinent in CRS [35]. Relaxin has been shown to reduce renal fibrosis in experimental animals [36].
Serelaxin is a recombinant form of human Relaxin 2. RELAX-AHF trial of Serelaxin recently demonstrated relief of dyspnea and reduced deaths at 180 days. In an international, double blind placebo controlled study in 1161 patients, Serelaxin infusion at 30ug/kg/day for 48 hours compared to a placebo resulted in improvement in dyspnea score by Visual Analogue Score-Area under the Curve (VAS-AUC) although there was a discordance with the other co-primary end point of dyspnea relief by Likert scale. Although the secondary end points of CV deaths or readmission for CHF or WRF did not differ between the groups, Serelaxin was associated with significantly reduced overall mortality at 180 days. The mean eGFR at study enrolment was around 53ml/min/1.73m2 (Stage 3 CKD) and more than 50% were in NYHA Class 3 or 4 CHF [37]. It was after a long time that improved survival was demonstrated in patients with ADHF with an intervention.
NEPRILYSIN-INHIBITOR IN CRS
Neprilysin is a naturally occurring neutral endopeptidase which degrades several endogenous vasoactive peptides like Natriuretic peptides (ANP/BNP), Bradykinin and Adrenomedulllin. Blocking Neprilysin leads to elevated levels of Natriuretic peptides and Bradykinin leading to natriuresis and vasodilatation [38].
In a recent large double-blind trial, Neprilysin inhibitor Sacubitril was combined with Angiotensin Receptor Blocker Valsartan to reduce the incidence of angioedema seen previously with ACE-inhibitor combination. 8442 patients with NYHA class ii-iv heart failure and an ejection fraction of 40% or less received either LCZ696 [Sacubitril +Valsartan as fixed dose combination in a dose of 200 mg (which delivers 160mg Valsartan)] twice daily or Enalapril (at a dose of 10 mg twice daily), in addition to recommended therapy. The primary outcome was a composite of death from cardiovascular causes or hospitalization for heart failure. The trial was terminated early at 27 months because the boundary of an overwhelming benefit with LCZ696 was crossed. There was a clear survival benefit and rehospitalisation rates were reduced by 21% with improved symptoms with LCZ696 [39]. LCZ 696 group showed higher proportion of hypotension and non-serious angioedema but lower proportion of WRF, hyperkalemia or cough. Of note, more than 3,000 patients in the study were in Stage 3 CKD with eGFR between 30-60ml/min/1.73m 2.
SUMMARY
The syndrome of CRS is complex in aetiology and poses enormous therapeutic challenges. The outcome for patients with CRS continues to be dismal with increased rehospitalisation and mortality. Renal function is the prime determinant of survival. Majority of randomized, controlled trials have belied the expectations raised by smaller studies for pharmacologic interventions and ultrafiltration. Two recent studies with Relaxin and Neprilysin inhibitor in combination with ARB are promising. After all the multiple negative studies, there might be a glimmer of hope for patients with CRS.
CONFLICT OF INTEREST
The author confirms that this article content has no conflict of interest.
ACKNOWLEDGEMENTS
Declared none.

